4 Application of a Posture and Movement Model in Practice This chapter presents an example a theoretical model as applied to intervention planning and implementation. The first section includes the source material for a posture and movement model. Findings from neuroscience and musculoskeletal studies are presented to explain and support components of the model. The second section presents the therapeutic principles of intervention for individuals with posture or movement impairments. These principles, derived from the source material, guide the choice and progression of intervention strategies for strengthening weak movement and postural systems. Learning Objectives Upon completing this chapter the reader will be able to do the following: • Define the differences in the anatomical features of the posture and movement systems. • Identify impairments associated with failure in one system and imbalance when both systems do not integrate. • Explain the physiological mechanisms that are operating when each system is active. • Translate the scientific findings to their practical application. • Apply therapeutic principles when designing and implementing intervention. • Progress from initial intervention to more demanding levels based on therapeutic principles. This chapter continues the process of applying theory to practice in the form of a model. This model of motor control defines the concepts of posture and movement and their application to intervention strategies. Source material from neurological and musculoskeletal fields forms the basis for proposing two distinctly different systems as components of the posture/movement model. The intent here is for the practicing therapist to see the relationship between basic sciences and clinical practice. The basic sciences give rise to the rationale for the options a therapist has in designing intervention activities. The options are presented in the form of therapeutic principles that are the rules of action. Principles are not laws, but they can be regarded as working hypotheses being tested. Each decision made in each intervention session of a given client can be more easily made when the rationale for that choice is clear. The posture and movement model translates into a method that can be used in intervention with clients having disorders of either or both posture and movement. Posture and movement represent two subsystems of motor control that are integrated to achieve coordination for functional tasks. The distinct roles of the subsystems are opposite in their goals, yet they are complementary when their interaction occurs in purposeful activity. The general nature of the postural system’s work is stabilization through maintenance of body position and orientation in space, maintenance of balance during movement, and modulation of the movement system. The general nature of the movement system’s work is to project the body or part of it through large excursions and to provide speed, especially in the responses of the limbs. The movement system mobilizes the body to move into space and acts upon the environment. A posture/movement model can also be defined as a stability/mobility model.1,2,3,4,5,6,7 Although the general concepts of posture and movement provide an overview, it is useful when assessing and providing intervention for people with impairments to have more detailed descriptions of the various functions of each subsystem. The subsystems in any one individual can be selectively damaged or both can be affected. The following are summaries of the subsystems functions. • The postural system provides the ability to maintain the upright position against gravity through vertical lift. • Postural responses also maintain the center of mass (COM) over the base of support (BOS) in two ways. First, in anticipation of movement that would place the COM outside the BOS, postural responses act to prepare the body to remain balanced. This anticipatory preparation occurs prior to the disturbance of posture and equilibrium by movement. Second, during the process of moving the COM, the postural system reacts with a compensatory balance response that maintains alignment. These reactive functions of the postural system are dynamic, involving small adjustments of the body on itself, but do not project the body from one place to another.6 • In addition to the whole-body responses, the postural system maintains the integrity of joint structure through active cocontraction of antagonistic muscles. When velocity or load is high enough to lead to mechanical instability of the joint, cocontraction increases dynamic joint stiffness to prevent damage. • The movement system is a primary controller when a wider range and a faster speed of motor responses are required. • To initiate fast responses, the movement system will recruit the high levels of tension required to overcome inertia. • Although axial regions do not have the same wide excursions in many functional tasks that the limbs do, their range in transitional activities can signal the need for a movement component. • In distal and rostral areas, rapid alternating patterns require the full participation of the movement system. The term mobility describes the goal of the movement system and is used here in a different way than when describing the independence of the whole individual moving in the environment. The anatomical support for the model begins with a description of the gross characteristics of skeletal muscles that identifies them as being more suited for either postural activity or movement, as seen in Table 4.1.10 This categorization is not an exact dichotomy because many muscles can function in both systems depending on the task and the context of the action. Table 4.1 Characteristics of muscles better suited for either postural or movement activities
4.1 Introduction
4.2 A Posture and Movement Model
4.2.1 General Concepts
4.2.2 Distinct Roles of Subsystems
Functions of the Postural System
Functions of the Movement System
4.2.3 The Anatomical Basis for the Posture and Movement Model
Gross Characteristics of Muscles
Characteristic | Muscles better suited for postural activities | Muscles better suited for movement activities |
Overall shape | Bipennate or multipennate | Fusiform |
Fiber orientation | Oblique in relation to axes | Parallel to long axis |
Length of fibers | Shorter | Longer |
Attachments | Broad and aponeurotic | Small and tendinous |
Location | More proximal, medial, deeper | More distal, lateral, superficial |
Number of joints crossed Location | One | Two or more |
Type of contraction | Cocontraction | Reciprocal |
Speed and extent | Small excursion, holding | Wide excursion, high velocity |
General function | Stability | Mobility |
Clinical Observation #1
Function
Maintenance of alignment of the head and neck upright with a chin tuck position.
Clinical Picture
A patient has a forward head (as seen in Fig. 4.1) with the lower cervical region flexed and the upper cervical region and the atlanto-occipital joint extended so the chin is up. Often, heavy bands of superficial muscle on each side of the midline with a deep groove between can be seen in the neck posteriorly.
Posture/Movement Impairment
The deep intrinsic muscles of the neck (rectus capitis posterior major and minor, obliquus capitis inferior and superior, rectus capitis anterior and lateralis) are failing to stabilize the neck through cocontraction with the deep flexors. The head is being held up by the more superficial extensor movement muscles (i.e., semispinalis capitis, longissimus capitis, cervical parts of the sacrospinalis). Movement is restricted as the movement muscles adapt and become stiffer in an attempt to substitute for the nonfunctioning postural muscles. As the person attempts to bring the neck into a flexed position, there can be a sudden drop of the head with loss of all extensor activity.

Fig. 4.1 This child sits supported with a forward head posture, stabilizing with superficial neck muscles.
Clinical Observation #2
Function
Maintenance of the trunk and neck in an upright position in sitting.
Clinical Picture
A patient sits in a slumped, flexed position with the head up from neck extension in the high cervical region. The pelvis is in an extreme posterior tilt with the weight back on the sacrum. The spinous processes are prominent, especially in the thoracic area. When requested, the person might be able to sit erect but will come to sitting with an abrupt movement and be unable to hold the position for long, as seen in Fig. 4.2a, b.
Posture/Movement Impairment
The deep intrinsic extensor muscles of the trunk (multifidus, rotatores, interspinalis, intertransversarii) are failing to stabilize the trunk bilaterally. These muscles would usually pack the vertebra, filling in around the spinous process and making only the tip visible. If the movement trunk extensors (iliocostalis, longissimus, spinalis) are still active, it will be possible for the person to move into full extension, but these muscles will fatigue rapidly. On the anterior side, the transversus abdominis is failing to cocontract with the deep intrinsics, such as the multifidus.
Clinical Observation #3
Function
Stabilization of the scapula so that its movement participates in the normal glenohumeral rhythm.
Clinical Picture
At rest, the scapula is abducted so far that its lateral border can be seen in the axilla, and its medial border is winged. The scapula and the humerus appear to be fused when the patient moves the arm, as seen in Fig. 4.3.
Posture/Movement Impairment
The weak scapular adductors (especially the middle trapezius) cannot hold the scapula in a position where the serratus anterior can be kept on a stretch. As the adductors become overstretched and the scapula abducts widely, the serratus anterior is unloaded, loses its ability to contract, and the scapula wings. This combination of the loss of active adduction and abduction removes a dynamic postural response that is required for the next in-line stabilization of the humerus through cocontraction at the glenohumeral joint. The movement system attempts to stabilize the joint; however, the response is not cocontraction of the rotator cuff muscles but fixation by more superficial muscles. The infraspinatus and the posterior deltoid, as part of the postural extensor pattern, are also weak and overstretched, leading to internal rotation of the humerus.
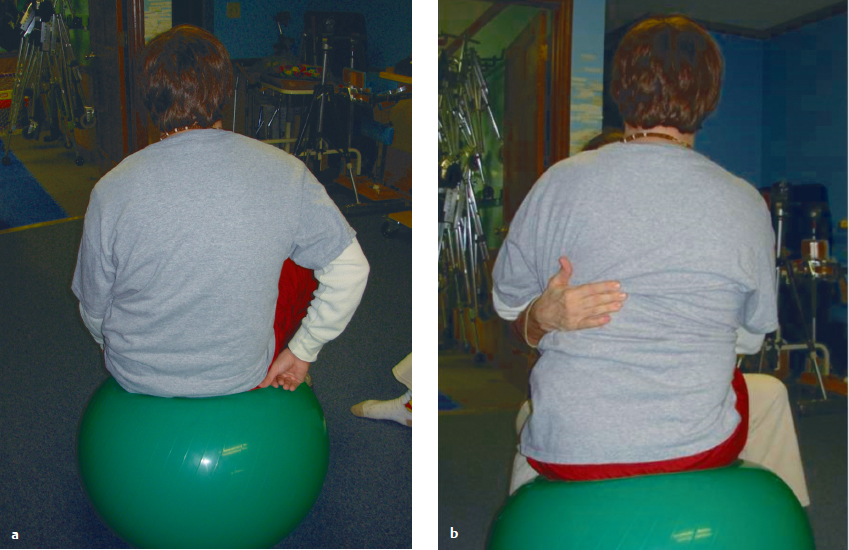
Fig. 4.2 (a, b) Young adult demonstrating usual sitting with rounded back. He is unable to hold full extension, although he can hold with cueing momentarily.
Clinical Observation #4
Function
Maintaining the upright position in the lower extremities during standing.
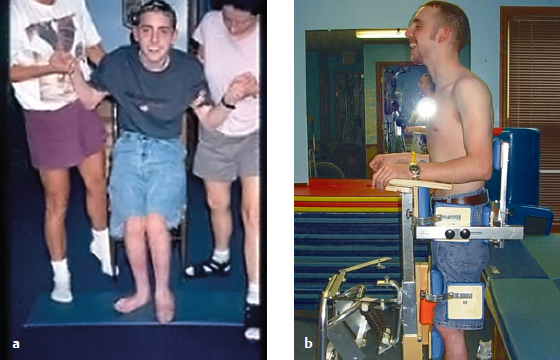
Clinical Picture
The patient is able to stand only with the hips and knees in flexion. During ambulation, the flexed posture continues.
Posture/Movement Impairment
Postural extensor muscles should be able to respond to stretch from the pull of gravity in their shortest range. This postural response means that the postural hip extensors, gluteus maximus, knee extensors, and vasti of the quadriceps should be able to hold in full extension. When they are weak, the set point for that response can be in a longer range. The patient sinks down until those muscles hit the longer set point, as seen in Fig. 4.4a. This patient might be able to come to full extension as seen in Fig. 4.4b but will have to use the movement system to do so. The result will be rapid fatigue and a return to the flexed position.

Fig. 4.3 Child demonstrat ing scapular abduction with insufficient stabilization on thoracic wall.
Muscle Fibers and Motor Units
Support for the posture/movement model also comes from the examination of different types of muscle fibers and motor units of skeletal muscles. Lieber11 has pointed out that several schemes for classifying muscle fiber types have been developed. He proposes that the most useful scheme is one based on physiological, biochemical, and morphological measures.
The three groups of muscle fibers are fast glycolytic (FG), fast oxidative glycolytic (FOG), and slow oxidative (SO). When glucose is oxidized in the absence of oxygen, glycolysis occurs. The anaerobic contractions that result cannot last much longer than 10 to 30 seconds.11 When glucose is metabolized in the presence of oxygen, oxidative phosphorylation occurs. This aerobic form of metabolism is more efficient than glycolysis.
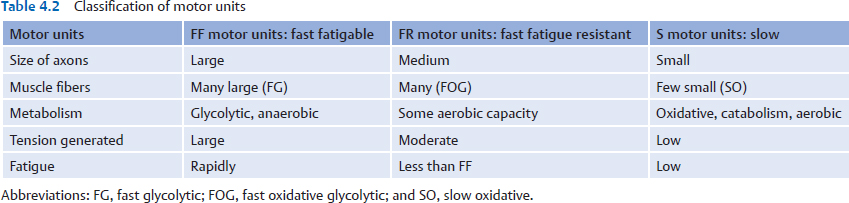
Motor units can also be classified based on the physiological properties of their muscle fibers, as seen in Table 4.2. A motor unit consists of an α-motor neuron and all the skeletal muscle fibers it innervates.
In terms of the posture/movement model, the SO motor units would be more appropriate for postural activity that requires sustained contractions with low levels of fatigue. The fast fatigable (FF) units would allow brief fast excursions of the limb where high tension was needed to overcome inertia and impart momentum. Fast fatigue resistant (FR) units would be needed where the activity was fast, repetitive movement.
Medial and Lateral Descending Motor Organization
Well before and into the 20th century, the motor system was defined by two supposedly independent systems: pyramidal and extrapyramidal. This classification is questioned as a basic organizational scheme because it does not include structures that are important parts of the motor system (i.e., the cerebellum, brainstem nuclei, and red nucleus). In addition, pyramidal and extrapyramidal structures are extensively interconnected. From an applied view, this classification does not provide the foundation for therapeutic intervention for disorders of motor control. The terms are still used in some neurology contexts.
In 1963, Kuypers12 proposed a different model of organization for the motor system based on the position of motor neurons in the spinal cord and the descending pathways that terminate there. His work continued as he collaborated with Lawrence13,14,15 to define the details of the model, which he presented again at a later time.16
Spinal Cord Organization and Descending Pathways
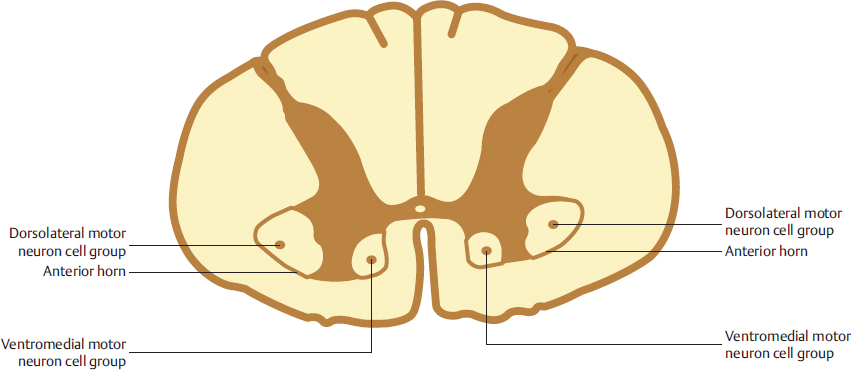
The pools of motor neurons (motor nuclei) in the anterior horn of the spinal cord are organized along a medial to lateral axis as seen in Fig. 4.5. The most medial motor neurons innervate the muscles of the neck and trunk (axial), and the most lateral motor neurons innervate muscles of distal regions (limb). Between these two groups are the motor neurons that innervate the proximal muscles (girdle). A ventral/dorsal gradient of organization has also been identified so that the cell groupings are often referred to as ventromedial and dorsolateral.
Descending Pathways
The descending pathways controlling the motor nuclei are divided into two main groups: medial (Fig. 4.6a, b) and lateral (Fig. 4.7a, b).16,17 All the pathways in the medial system have a bilateral influence on axial and proximal functions. The medial pathways of the brainstem are the pontine reticulospinal, the vestibulospinal (medial and lateral), and the tectospinal tracts. These pathways terminate on interneurons in the ventromedial part of the intermediate zone of the spinal cord and on the medial motor neurons. The interneurons connect bilaterally to the medial motor neurons that innervate axial and proximal muscles.
The lateral pathways have a contralateral influence on distal functions.
Integrated Functions of the Subsystems
As described in the introduction to this section, the two subsystems have roles that are opposite and yet complementary when integrated for purposeful activity. Examples of this integration follow.
• The accuracy of limb placement is dependent not only on the movement system activity for projection but also on the postural system providing cocontraction as well as synergistic activity related to the pattern of movement. The variability of end range placement is directly related to the postural system guidance.8
• Patterns of new motor learning manifest excessive recruitment, which gradually reduces with development of skill.8,9 When a subject is learning a novel movement, cocontraction is greater at the beginning and gradually reduces over the course of acquisition. This excessive cocontraction is often seen as a form of fixation called in to prevent excessive movement. It would appear that refinement of motor functions occurs as selection of necessary movement components is accompanied by more exact postural guidance to overcome excessive degrees of freedom.
• Transitions from one posture to the next, as in rolling over, moving supine to sit or sit to stand, and walking and running, require the integration of the movement and posture systems. The large excursions of movement and, in some cases, the speed of movement require the functions of the movement system. At the same time, the postural system is needed to maintain balance and orientation during the transitions.
Effects of Lesions of Medial and Lateral Systems
The separate functions of the medial and lateral systems can be illustrated by the effects of selected lesions that dissociate the systems. Lawrence and Kuypers undertook extensive studies of the descending pathways of the medial and lateral systems in monkeys.14,15 When the corticospinal tract was interrupted bilaterally, the monkeys lost individual finger movements permanently and “all movements were slower and fatigued more rapidly than in the normal animal.”14 The lateral corticospinal tract is part of the lateral system. If the lateral system provides not only control of distal functions but also speed for all movements, then it could be part of the system for the movement part of the posture/movement model presented in this chapter. The animals with destruction of the corticospinal system (lateral motor system) retained their ability to maintain posture and to balance (medial motor system).
When the medial brainstem pathways were interrupted bilaterally, the animals were unable to right themselves and demonstrated a severe deficit in axial and proximal limb functions. “When sitting they tended to slump forward, with shoulders elevated and the arms flexed at the elbows and adducted to the trunk.”15 The medial pathways provide the innervation for the axial and proximal regions of the body. The medial system can be considered the controlling system for the postural part of the posture/movement model presented in this chapter.
Related posts:
 The Practice of Speech-Language Pathology from a Neuro-Developmental Treatment Perspective
The Practice of Speech-Language Pathology from a Neuro-Developmental Treatment Perspective
 Report B5 Enhancing Functional Independence in a 10-Year-Old Boy with Cerebral Palsy, Spastic Quadriparesis
Report B5 Enhancing Functional Independence in a 10-Year-Old Boy with Cerebral Palsy, Spastic Quadriparesis
 Report B3 Development of an Intervention Plan of Care for a Young Child with Hemiplegia
Report B3 Development of an Intervention Plan of Care for a Young Child with Hemiplegia
 Neuro-Developmental Treatment Practice Model
Neuro-Developmental Treatment Practice Model
 Report B8 Providing Ongoing Neuro-Developmental Treatment–Based Physical Therapy Intervention for a Medically Fragile Child with Severe Disabilities
Report B8 Providing Ongoing Neuro-Developmental Treatment–Based Physical Therapy Intervention for a Medically Fragile Child with Severe Disabilities
 Neuro-Developmental Treatment Intervention—A Session View
Neuro-Developmental Treatment Intervention—A Session View
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


