38 Approach to Pediatric Electromyography
Maturation Issues
• Conduction velocities less than 75% the lower limit of normal
• Distal latencies and late responses greater than 130% the upper limit of normal
• Conduction block, which signifies not only demyelination but acquired demyelination
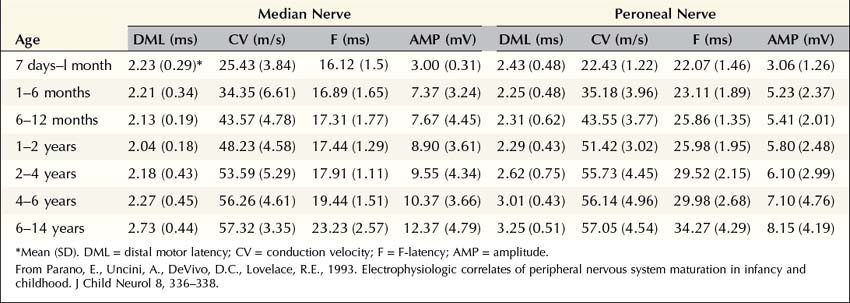
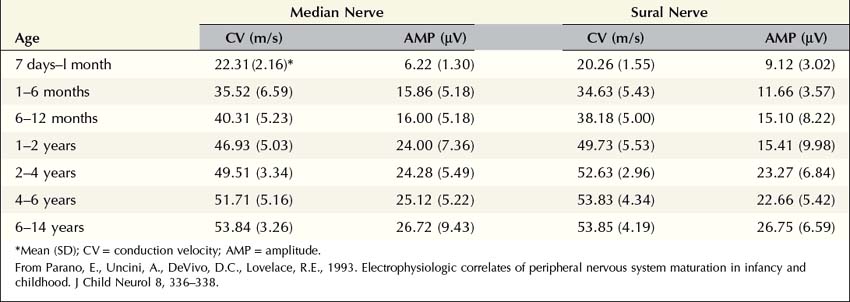
However, infants and young children often have slowed conduction velocities that would be considered in the “demyelinating range” for adults. In most cases, this is not because infants and young children have demyelinated nerves; rather, they have nerves that have yet to be myelinated in the first place. The process of myelination is age dependent, beginning in utero, with nerve conduction velocities in full-term infants approximately half that of adult normal values. Accordingly, nerve conduction velocities of 25 to 30 m/s are normal at birth. Conduction velocity rapidly increases after birth, reaching approximately 75% of adult normal values by age 1 year, and the adult range by age 3 to 5 years, when myelination is complete. Accordingly, when a child is studied in the EMG laboratory, it is essential that age-based normal control values are used (Tables 38–1 and 38–2).
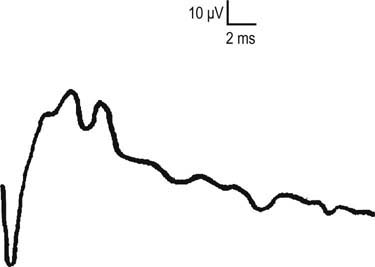
One interesting aspect of myelin maturation is often observed during the nerve conduction studies. Many are familiar with the fact that different white matter tracts in the central nervous system myelinate at different times. Indeed, one can often use the pattern of myelination on a brain magnetic resonance imaging (MRI) scan to correctly predict the age of a young child. Similarly, different fibers in the peripheral nervous system myelinate at different times as well. In the EMG laboratory, this often manifests as a bifid morphology (i.e., two separate peaks) on sensory nerve action potentials (SNAPs) in infants and children (Figure 38–1). This bifid morphology is due to some fibers having already been fully myelinated (the first peak), whereas others have not and trail behind (i.e., the second peak). It is not unusual to see bifid SNAPs between the ages of 3 months and 4 to 6 years. These bifid SNAPs are a completely normal finding. Eventually, as the fibers in the second peak fully myelinate, the second peak moves to the left and merges with the first peak. This forms a larger sensory response, as is typically seen in adults.
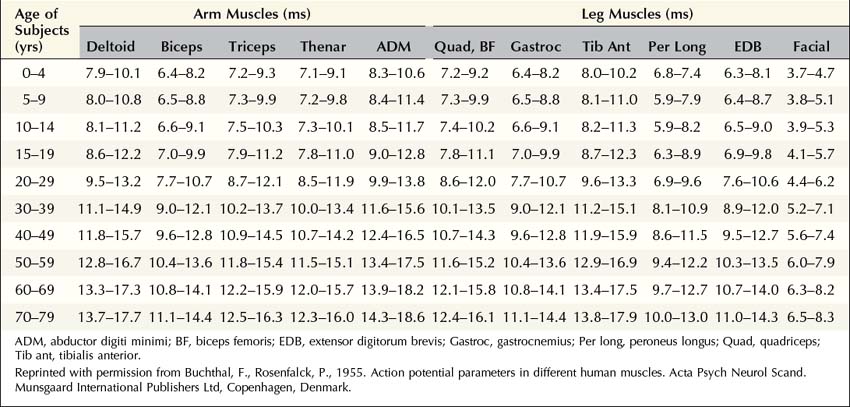
The most important maturation issue for the needle EMG portion of the examination is the size of the motor unit. It is no surprise that the physical size of a motor unit of a newborn is much smaller than that of an adult. Transverse motor unit territory increases greatly with age, doubling from birth to adulthood, mostly because of the increase in individual muscle fiber size. Thus, normal motor unit action potentials (MUAPs) in infants typically are very small, representing the physical size of the motor unit. Indeed, in infants, it often is difficult to differentiate normal MUAPs from myopathic ones. This once again underscores that when one interprets EDX findings in children, including MUAPs, it is essential to use age-based normal control values (Table 38–3).
Technical Issues
Second, smaller electrodes often are needed in infants and young children because their limbs and muscles are so small. The typical bar electrode that has the active and reference contacts separated by 2.5 cm often is too large for most infants and small children (Figure 38–2). Standard 10 mm disc electrodes often will suffice for most ages, except for newborns in which smaller electrodes generally are needed. Likewise, the standard adult stimulator often is too large for infants and young children because of the size of the prongs and the distance between the cathode and anode. Often it is preferable to use a pediatric-sized stimulator so that the nerve of interest is more accurately stimulated (Figure 38–3).


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


