Carlo Alberto Tassinari
Roberto Michelucci
Hideo Shigematsu
Masakazu Seino
Introduction
Atonic and myoclonic–atonic seizures represent specific seizure types whose definition implies a characteristic physiopathologic mechanism and a well-defined electro-clinical pattern that may be demonstrated only by polygraphic and video-polygraphic recording. Therefore, these seizures cannot be diagnosed only on the basis of the clinical history, which may usually reveal recurrent “falling” seizures, associated or not with minor motor events. Falling seizures, otherwise termed epileptic drop-attacks or astatic seizures,5 are a heterogeneous group of epileptic seizures in which the fall represents the main or only clinical feature, with no major motor phenomena (e.g., convulsions) occurring.58,82 Falling seizures may represent a variety of seizure types (either generalized or focal) and mechanisms, including widespread myoclonic jerks, tonic contraction, pure atonic events, or the combinations of motor phenomena, as in the case of myoclonic–astatic seizures. These observations may explain the controversies in the terminology of epileptic falls and the high number of terms used in the past (akinetic, atonic, astatic, static, drop, apoplectic, inhibitory).
History
Seizures characterized by a sudden fall have been known for a long time. Apart from early clinical notes by Tissot and Newman dating back to the 18th and 19th centuries, respectively, the first detailed description of atonic seizures was given by Hunt in 1922, who called the condition “static epilepsy”—that is, a “form of epilepsy characterized by sudden losses of postural control.”40 In 1945, Lennox proposed the term akinetic seizures for attacks of this type, which he rebaptized astatic in 1951.47,48 These seizures were considered to belong to the electro-clinical group of petit mal absences: Lennox suggested the term petit mal triad to include absences, myoclonic jerks, and akinetic attacks.49 In 1966, Gastaut et al.29 described the Lennox-Gastaut syndrome, in which falling seizures were a characteristic seizure type, and also reported a few cases of polygraphically studied atonic seizures.30 In the same years, there was the first polygraphic demonstration of a specific seizure type with a combination of myoclonus preceding atonia, which was termed myoclonic–astatic seizure by Kruse.42 In 1981, the Commission on Terminology and Classification of the International League Against Epilepsy (ILAE) established the term atonic seizure for falling attacks with loss of tone.11 Last, in 2001, the Task Force on classification and terminology of the ILAE included atonic seizures and myoclonic–atonic seizures within an accepted list of generalized seizures.24
Definitions
Atonic seizures are currently defined as epileptic attacks characterized by a sudden loss or diminution of muscle tone, which may be confined to a segment (limb, jaw, head), or involve all postural muscles, leading to a slumping to the ground.5,11,28 In atonic seizures, the loss or diminution of muscle tone is “pure,” without apparent preceding myoclonic or tonic events.5
Myoclonic–atonic seizures may be defined as epileptic attacks in which the atonia is preceded by a myoclonic jerk (i.e., a sudden and brief—<100 msec—involuntary contraction of muscle groups of variable topography).5
In the recent glossary of descriptive terminology for ictal semiology,5 it has been also stated that “falling seizures” are better termed astatic, this term implying “loss of erect posture that results from atonic, myoclonic or tonic mechanism”; drop attack would be a synonym.
Epidemiology
Because of controversies in terminology and the need of a polygraphic recording to perform a reliable diagnosis, exact figures for the incidence of these seizure types are not available. Atonic seizures have been quoted to occur in at least 50% of cases of Lennox-Gastaut syndrome and probably in 2% to 3% of an epileptic population.60 However the introduction of video-polygraphic systems in the analysis of “astatic” seizures has clarified that seizures characterized by pure diminution or loss of tone (atonic seizures) are distinctly rare, accounting for only a minority of epileptic drop attacks. Gastaut et al.30 found atonic seizures only in 3 out of 2,000 epileptic patients followed at the Centre St. Paul in Marseille. Myoclonic astatic seizures are likely to reflect the prevalence of myoclonic–astatic epilepsy, accounting for 1% to 2% of all childhood epilepsies.17
Anatomic pathways and pathophysiology
Because of the variety of seizures featuring atonia as the main clinical and polygraphic event, it is likely that different mechanisms are implicated, involving cortical and subcortical structures.
Gastaut and Broughton27 considered “epileptic drop attacks” to be related to very brief but intense inhibitory mechanisms, suggesting the importance of motor cortex participation. Data from electrical stimulation of human cerebral cortex reveal the existence of frontal regions whose activation produces inhibition of voluntary movement.52,53,54 These regions, defined as “negative motor areas”, have been localized in the superior bank of the sylvian fissure near the
rolandic representation of the face (“primary negative motor area”)52,70 and in the rostral portion of the supplementary motor area (SMA), in a region immediately anterior to the primary motor cortex (“supplementary negative motor area”).50 The importance of these cortical inhibitory areas is well established in the genesis of focal atonic seizures and negative myoclonus72,76,84 but is only presumed in the origin of atonic falling seizures.75 An alternative explanation is that epileptic discharges in the primary sensorimotor cortex can produce negative motor phenomena via direct inhibition of the spinal motoneuron pool, as suggested in humans by means of direct cortical stimulation through subdural electrodes36 or ictal electrocorticogram.55
rolandic representation of the face (“primary negative motor area”)52,70 and in the rostral portion of the supplementary motor area (SMA), in a region immediately anterior to the primary motor cortex (“supplementary negative motor area”).50 The importance of these cortical inhibitory areas is well established in the genesis of focal atonic seizures and negative myoclonus72,76,84 but is only presumed in the origin of atonic falling seizures.75 An alternative explanation is that epileptic discharges in the primary sensorimotor cortex can produce negative motor phenomena via direct inhibition of the spinal motoneuron pool, as suggested in humans by means of direct cortical stimulation through subdural electrodes36 or ictal electrocorticogram.55
Gloor32 stressed the importance of recurrent cortical inhibition (mediated via the thalamocortical volleys) leading to interference with cortical function during the spike-and-wave discharges (SWDs) of absence seizures. Oguni et al.64 suggested that atonic seizures associated with generalized SWDs may have a neurophysiologic mechanism in common with absence seizures, with the atonic phenomenon being only the expression of a stronger disruption of cortical activity.
The good results of callosotomy in the treatment of epileptic drop attacks in the context of partial epilepsies suggest that bilateral synchronization of the epileptic discharge via the corpus callosum is a crucial mechanism.65 Whether this may lead to a bilateral activation of inhibitory cortical areas or of cortical regions projecting downward to brainstem structures is not known.
The brainstem has also been considered to play a role in the origin of atonic seizures, both generalized and partial.10,23,41,89 In the brainstem, the direct or indirect (via the corticoreticular efferents) activation of the pontomedullary reticular formation, which is responsible for atonia or inability to move in rapid eye movement (REM) sleep and in cataplexy, could produce a motor inhibition and underlie atonic seizures.44
Electroclinical features
Atonic and myoclonic–atonic seizures have been mostly documented in large clinical series of generalized epilepsies of infancy, such as Lennox-Gastaut syndrome or myoclonic astatic epilepsy.
Gastaut et al.30 studied the electroclinical features of 300 “effondrements epileptique” by using video-polygraphic methods in three young patients with Lennox-Gastaut syndrome. Egli et al.23 recorded 239 “drop seizures” both by radiotelemetered electroencephalographic (EEG) split-screen videotaping and polygraphically in 45 patients suffering from “secondary generalized epilepsy.”
Similarly, Ikeno et al.37 recorded 48 epileptic falls in 15 children, captured by a self-tracking video monitoring system. Oguni et al.62 studied 36 drop seizures in five patients with myoclonic–astatic epilepsy of early childhood with simultaneous split-screen video recording and polygraph. By using the same technique, Yaqub90 also recorded falling seizures in 21 patients with Lennox-Gastaut syndrome.
Dravet et al.20 reported the various types of epileptic drop attacks in eight children whose seizures were recorded by polygraphy and simultaneous video.
Oguni et al.63 described the video-EEG (V-EEG) and video-polygraphic findings of myoclonic, atonic, and myoclonic–atonic seizures in 30 children with myoclonic–astatic epilepsy.
The analysis of these studies has clarified some of the complexities of the falling or astatic seizures, which have been found to encompass four different seizure types: pure atonic seizures, myoclonic–atonic seizures, myoclonic seizures, and tonic seizures (including axial spasms).77,82.
Moreover atonic seizures may have a generalized or focal origin.
Generalized Atonic Seizures
Clinical Features
Only a few polygraphically documented atonic seizures are available in the literature: atonic seizures were present in one of 15 children studied by Ikeno et al.,37 in nine of 45 patients observed by Egli et al. with epileptic falls,23 in 10 of 30 patients studied by Oguni et al.,63 and in three children described by Gastaut et al.30
From clinical observation, two forms of atonic seizures have been recognized30
Brief atonic seizures (also called effondrements epileptiques), in which loss of tone may be restricted to the head (head drop) or involve all postural muscles, leading to a slumping to the ground. If consciousness is lost, this loss is extremely brief. The patients are able to stand up immediately after the fall.
Prolonged atonic seizures (also called akinetic seizures), in which the loss of consciousness and the generalized atonia last for 1 to several minutes. The patient falls to the ground and remains mute and motionless.
Gastaut et al.30 studied the clinical features of the brief atonic seizures by video recording and found that the patients fall to the ground in less than 1 second, with a typical sequence of events being (a) head drop (lasting for 250 msec) and (b) trunk and legs drop (from 250 to 800 msec) (Fig. 1).
After an intermediate period of about 1 second, patients recover a normal standing position in about 2 seconds. Oguni et al.,62 by examining the video-polygraphic features of 69 “atonic epileptic drop attacks” recorded in two patients with myoclonic–astatic epilepsy, observed that the clinical manifestations ranged from collapsing and landing on the buttocks to head nodding only. Detailed video analysis of the drop attacks with the patient in standing position demonstrated the first manifestations to be flexion at the waist and knees, followed by further knee flexion, leading to falling straight down and landing on the buttocks. More recently, the same authors recorded atonic seizures in 11 children while they were either in a sitting or standing position.63 When in a standing posture, patients fell straight downward, landed on their buttocks, and recovered immediately. When sitting, the patients fell forward or backward depending on the position of their center of gravity. The polygraphs, corresponding to the atonic seizures, showed sudden interruptions of ongoing electromyographic (EMG) potentials confined to the upper trunk when seizures were mild, and extending to the lower antigravity muscles when they were intense. The duration of EMG silence extended to 400 msec, which indicated rapid recovery, either immediately after or possibly during the fall.
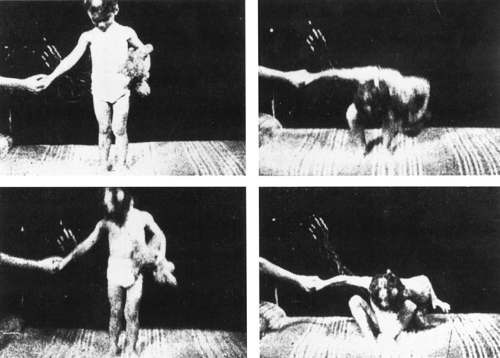 FIGURE 1. Brief atonic seizures (“effondrement atonique epileptique”). Video recording of a very brief atonic seizure, showing a typical sequence of events: initial head drop (left) and subsequent trunk and leg drop (right). It is interesting to note that the fall occurs exactly on the body axis, and the arms are not involved by tonic or myoclonic phenomena. These features may help in identifying an epileptic atonic fall on direct clinical observation. From Gastaut H, Tassinari CA, Bureau-Paillas M. Etude polygraphique et clinique des “effondrements atoniques epileptiques.” Rev Neurol. 1966;36:5–21, with permission. |
Electroencephalographic Findings
Interictal EEG findings are not specific and consist of bursts of slow spike-and-wave activity or polyspike-and-wave (PSW) complexes.
The ictal EEG of atonic seizures discloses a generalized PSW discharge, with loss of tone usually being associated with the slow wave component of the spike-and-wave complexes (Figs. 2A, 3, and 4). Other ictal patterns include low- or high-voltage fast activity, flattening, or a burst of polyspikes followed by generalized spike-and-wave activity. Polygraphic recording may reveal additional subtle clinical signs, such as bradycardia or brief arrest of respiration.
Generalized Myoclonic–Atonic Seizures
Clinical Features
Myoclonic–atonic seizures represent the main seizure type in myoclonic–astatic epilepsy of early childhood of Doose,16,18,21 and are probably more frequent than previously believed (see Chapter 232). These seizures have been documented in nine of 45 patients studied by Egli et al.,23 in three of 15 children reported by Ikeno et al.,37 and in four of 21 patients described by Yaqub.90 They have also been reported in detail by Gastaut and Broughton27 and Dravet et al.20
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


