Cervical Myelopathy: Laminectomy
Nancy E. Epstein
Cervical laminectomy is a valuable treatment modality for the surgical management of congenital or acquired multilevel cervical spinal stenosis often associated with disk herniations, spondylosis, ossification of the posterior longitudinal ligament (OPLL), and ossification of the yellow ligament (OYL) with progressive myelopathy. The cervical lordotic curvature must be preserved in these surgical patients, and where instability is present and/or threatened, a dorsal facet wiring and fusion or lateral mass fusion should also be performed.
ANATOMY
The spinal cord and nerve roots may become compressed in a canal narrowed in its anterior-posterior (AP) dimensions by absolute or relative stenosis, other forms of stenosis associated with congenitally shortened pedicles (Achondroplasia), and lowered laminar arches (1). The normal AP diameter of the spinal canal between the C3-C7 levels is 17 mm. In absolute (congenital) stenosis, the canal is narrowed to 10 mm or less, while in relative (acquired) stenosis, it measures approximately 13 mm (2). The requisite AP dimension of the spinal cord of 0.8 to 1.3 cm, and the 2 to 3 mm occupied by the soft tissues structures (posterior longitudinal ligament, yellow ligament, epidural fat, venous plexus), leaves little to no residual “available space” for the neural tissues (1). Disk disease, spondyloarthrosis, and hypertrophy or ossification of the posterior longitudinal and/or yellow ligaments further contribute to radicular and myelopathic compression syndromes. Although, chronic microtrauma(s) may contribute to slow progressive adverse changes to the spinal cord parenchyma, and acute hyperextension injury can result in the rapid evolution of irretrievable cord damage.
PATHOLOGY
In spinal stenosis, at least two major mechanisms of neural injury are invoked: direct mechanical compression and indirect vascular insufficiency. These two processes contribute to a varied extent and location of spinal cord changes often located several levels proximal or distal to sites of maximal compression. In cadaveric models, atrophy, demyelination, and vascular infarction involving gray and white matter (ascending and descending long tracts) occur far removed from major sites of disk, spondylotic, or OPLL.
CLINICAL PRESENTATION
Patients with absolute stenosis typically present in their forties or fifties, while those with relative stenosis with secondary acquired spondyloarthrosis become symptomatic in their sixties or seventies. Males outnumber females in a 2:1 ratio. While some patients exhibit radiculopathy alone, the majority present with myelopathy with or without radiculopathy, with the AP diameter of the canal narrowed by over 50%.
Myelopathy may be rated using different grading systems. In Japan and Asia, the Japanese Orthopaedic Association Score assigns 17 points to both upper and lower extremity function (3,4). In the United States and Europe, the Nurick Myelopathy Grading System is often utilized: grade 0—intact, grade I—mild myelopathy, grade II—mild-moderate myelopathy, grade III—moderate myelopathy, grade IV—moderate to severe myelopathy, and grade V—severe myelopathy. Most patients undergoing laminectomy with or without posterior fusion present with moderate to severe myelopathy (Nurick grades III to IV). Neurologic deficits in the upper extremities are characterized by the “useless hand syndrome,” including diffuse atrophy, weakness of the hands, loss of dexterity, and frequent superimposed cephalad radicular deficits (C4, C5). Proximal lower extremity weakness may also be associated with severe cervical myelopathy, with intrinsic cord changes being corroborated by neurologic evidence of ataxia, spasticity, hyperreflexia, and bilateral Babinski responses. Accompanying sensory deficits may include numbness and loss of proprioception, impaired vibratory appreciation, and varying sensory levels. Changes in the lower extremities reflect underlying dorsal column dysfunction, characterized by a positive Romberg sign and
inability to walk in a tandem fashion. Sphincter function is compromised only late in the clinical course.
inability to walk in a tandem fashion. Sphincter function is compromised only late in the clinical course.
DIFFERENTIAL DIAGNOSES
Differential diagnostic considerations for cervical myelopathy include multiple sclerosis (MS), amyotrophic lateral sclerosis (ALS), paraneoplastic syndromes, toxic-metabolic disorders (diabetes, alcoholism, B12 deficiency), and others. When considering MS, 8% of brain MR scans demonstrate demyelinating plaques; cerebrospinal fluid (CSF) evaluations may show monoclonal bands, myelin-based protein, and gamma globulin. Electromyography (EMG) may diagnose ALS and peripheral neuropathy, while blood tests may document other metabolic disorders. Of interest, 10% of patients with lumbar stenosis will exhibit tandem coexistent cervical cord compression and may or may not be sufficiently myelopathic to warrant initial cervical decompression.
BIODYNAMICS
FLEXION AND EXTENSION X-RAYS
Flexion and extension maneuvers themselves, in addition to radiographic findings, alter the conformation of the cervical spinal canal and cord (1). Although the spinal canal enlarges in flexion, increased axial tension narrows the AP diameter of the spinal cord, deforms the lateral columns/anterior horns, and may contribute to ischemia. Alternatively, hyperextension narrows the spinal canal, widens the cord, and promotes inward shingling of the yellow ligament and laminae, reducing the overall available space; cord perfusion may be increased with release in axial tension.
MONITORING OF CERVICAL SURGERY
CONTINUOUS INTRAOPERATIVE SOMATOSENSORY EVOKED POTENTIAL MONITORING
Intraoperative somatosensory evoked potential (SEP) monitoring involves the continuous evaluation of median or ulnar and posterior tibial potentials throughout the duration of surgery, and should be utilized in conjunction with electromagnetic motor evoked potentials (MEP), and EMG monitoring (5). This technique is noninvasive and should be performed continuously for patients before, during, and after laminectomy with or without attendant fusion. Monitoring both ulnar and posterior tibial (upper and lower extremity) potentials is critical to avoid significant intraoperative cord damage. Potentials are monitored using skin electrodes applied along the median or ulnar aspect of the wrist, and over the posterior tibial nerve at the level of the medial malleolus of the ankle, and are recorded over the somatosensory cortex. Significant changes are defined by over 50% loss of amplitude or greater than 10% prolongation of latency. If significant changes occur, both medical (increased oxygenation, decreased inhalation or intravenous anesthetic, warming of irrigating solutions, induction of hypertension, addition of peroxide to hyperoxygenate a wound) and surgical (decrease or release of distraction, cessation of manipulation) resuscitative measures may be invoked. It is important to avoid the use of porcine skin gelatin (Gelfoam, Pfizer, NY) into confined spaces where they may expand (can absorb several times their weight in blood) and contribute to neurologic compromise (cord or root compression, arachnoiditis, pain, sphincter dysfunction) and increased infection/abscess/meningitis rate, allergic reactions, and others.
RELATIVE HYPOTENSION PRECIPITATING SEP LOSS
When previously performing cervical laminectomies in the seated position, significant parallel SEP amplitude and latency changes signaled a “relative hypotension” or enough of a drop in blood pressure to compromise cord perfusion. In these instances, induction of hypertension (20% to 30% above baseline) became warranted. Only rarely is “relative hypotension” with resultant somatosensory evoked potential (SSEP) changes seen in the prone position; in these instances, resolution of the changes will occur with appropriate elevation of the systemic blood pressure, thus avoiding a permanent deficit.
INTRAOPERATIVE ELECTROMYOGRAPHIC MONITORING
EMG monitoring should be considered during operative positioning and critical phases of intraoperative nerve root manipulation. When a foraminal disk is being excised during a laminectomy, EMG changes may signal root compromise. During fusions, too much tension on the construct may precipitate EMG changes and require procedure modification.
INTRAOPERATIVE MAGNETIC MOTOR EVOKED POTENTIAL MONITORING
MEPs may also be employed intraoperatively to supplement but not supplant SSEPs. MEPs provide direct evaluation of the anterior motor pathways and are critical when resecting ventral cord pathology with SSEPs typically reflecting posterior column dysfunction.
NEURODIAGNOSTIC STUDIES
PLAIN X-RAYS
On a 6-foot lateral plain film, one may directly measure the AP diameter of the spinal canal (normally 17 mm). The presence of stenosis on a plain x-ray may also be determined by observing where the posterior margin of the facet joints intersects the dorsal interlaminar line: (a) if these two lines are directly superimposed, significant stenosis exists and (b) if not, stenosis is typically absent or less severe. Additionally, if the width of the vertebra does
not fit within the AP diameter of the canal, canal stenosis is typically present. Stenosis can also be further confirmed on MR- and CT-based studies.
not fit within the AP diameter of the canal, canal stenosis is typically present. Stenosis can also be further confirmed on MR- and CT-based studies.
LORDOSIS, KYPHOSIS
Optimal candidates for laminectomy or laminoplasty, with or without fusion, require adequate preservation of the cervical lordosis, or an exaggerated lordotic curvature, without kyphosis (Figs. 76.1 and 76.2). A lordotic curvature of at least 10 degrees is required to allow the cord to migrate away from ventrally situated osteophytes or OPLL if a dorsal decompression is to be successful (6). Ventral compression is relieved if there is a minimum of 10 degrees of lordosis and less than 7 mm of ventral OPLL, while less than 10 degrees of lordosis and more than 7 mm of ventral OPLL will result in residual ventral cord compression.
Instability on dynamic lateral radiographs consists of (a) greater than 3.5 mm of sublimation, (b) greater than 20 degrees of angulations, and (c) greater than 1 mm of motion between the tips of the spinous processes.
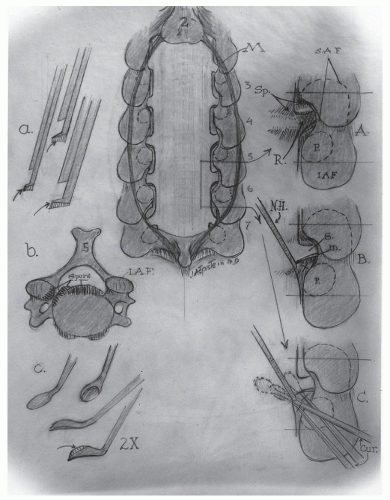 Figure 76.1. a: Kerrison punches are filed down to narrow the bite plate placed under the lamina. b: Ventral osteophytes cross the base of the cervical spinal canal. c: Small down-biting curettes are utilized to remove foraminal disks/spurs. A: Medial facetectomy foraminotomy decompresses the foraminal nerve root. B: Removal of foraminal disk/spurs requires gentle medial retraction of the root. C: Small down-biting curettes are utilized to remove foraminal disks/spurs. (Copyright owned by Dr. Nancy E. Epstein, drawn by Dr. Joseph A. Epstein.) |
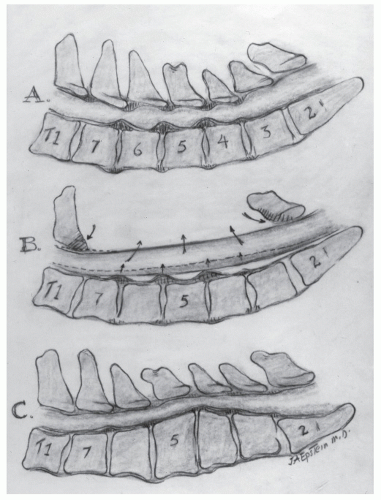 Figure 76.2. A: Congenial cervical stenosis accompanied by acquired anterior stenosis, characterized by ventral osteophytes and dorsolateral OYL. B: An adequate lordotic curvature allows for a laminectomy to adequately decompress the spinal canal. C: Kyphosis is a contraindication to laminectomy, as the cord would remain tethered over the ventral pathology. (Copyright owned by Dr. Nancy E. Epstein, drawn by Dr. Joseph A. Epstein.) |
MAGNETIC RESONANCE IMAGING (MRI)
MRI readily evaluates intrinsic cord and attendant soft tissue pathology in patients with cervical spondylotic myelopathy (CSM), OPLL, or OYL (5) (Figs. 76.3, 76.4 and 76.5). The sagittal, coronal, or transaxial images reveal maximal spinal cord and/or nerve root compression while also showing changes in cord signals. On T1-weighted images, the CSF remains hypointense, the vertebral bodies are isointense/hyperintense, and the cord appears isointense. On the T2-weighted images, CSF becomes hyperintense, thereby providing a “myelographic” effect, while increased cord signals are consistent with edema, myelomalacia, demyelination, or possibly intramedullary cystic necrosis or degenerative syrinx formation. The latter findings may constitute sufficient criteria to negate decompressive surgery as patients’ deficits are more likely permanent/irreversible. Of further interest, some studies show that increased cord signals on T2-weighted images for CSM patients were poor prognostic indicators, a finding not mirrored for OPLL patients. MR interpretations for degenerative cervical disease unfortunately
include the frequent underestimation of the bony pathology (spondylostenosis, stenosis, OPLL, OYL) due to the hypointense appearance (negative image) of the bone.
include the frequent underestimation of the bony pathology (spondylostenosis, stenosis, OPLL, OYL) due to the hypointense appearance (negative image) of the bone.
 Figure 76.3. This T2 sagittal MR study documents C3-C4 retrolisthesis, marked dorsolateral compression with inward shingling of the laminae at C3-C4 and C4-C5, and dorsolateral C2-C3 through C5-C6 OYL. Following a laminectomy of C4 and C5 with undercutting of C3 and C6 and posterior fusion C2-T1, the patient’s myelopathy resolved. |
 Figure 76.4. Case 1 This lateral MR T2-weighted image reveals a grade I-II subluxation at the C3-C4 level with severe ventral and dorsolateral compression. A C3 and C4 laminectomy with undercutting of the C2 and C5 laminae, accompanied by a posterior C2-C5/C6 fusion, was performed. Decompression relieved cord compression, while the C2-C5/C6 fusion stabilized the bilateral C3-C4 facet fractures and grade I-II C3-C4 olisthesis. |
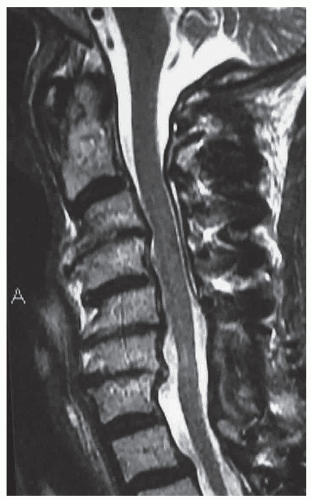 Figure 76.5. Case 2 In Case 2, following a C6 and C7 laminectomy for OYL and posterior C2-T2 fusion, the postoperative T2-weighted midline sagittal MR demonstrated atrophy of the cord (characterized by plentiful CSF around the cord) and residual increased signal in the cord tissue itself. |
COMPUTED TOMOGRAPHY (CT)
A major advantage of adjunctive CT-based studies is the ability to directly visualize (positive image) bony structures. Sagittal, coronal, transaxial, 2D, and 3D reconstructed images clearly demonstrate bony pathology (Figs. 76.6 and 76.7). In particular, OPLL is readily documented in all dimensions. Intrathecal contrast (myelo-CT) provides additional detail regarding cord or root compression. This study should be avoided in patients with severe cord compression or edema as this may lead to acute neurologic deterioration. Postoperatively, 2D and 3D CT-based examinations help confirm fusion progression by directly demonstrating (1) loss of lucency at
fusion site and (2) continuity of bone graft (e.g., between overlying bone graft and laminae/facet joints following laminectomy with posterior fusion).
fusion site and (2) continuity of bone graft (e.g., between overlying bone graft and laminae/facet joints following laminectomy with posterior fusion).
Related posts:
 Cervical Orthoses and Cranioskeletal Traction
Neurologic Examination: Grading Scales
Computed Tomography and Myelography of the Cervical Spine
Pediatric Spinal Cord Injury
Spinal Cord Injury: Assessment and Neurologic Classification
Subaxial Cervical Injuries: Current Concepts in Classification and Treatment
Cervical Orthoses and Cranioskeletal Traction
Neurologic Examination: Grading Scales
Computed Tomography and Myelography of the Cervical Spine
Pediatric Spinal Cord Injury
Spinal Cord Injury: Assessment and Neurologic Classification
Subaxial Cervical Injuries: Current Concepts in Classification and Treatment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


