CHAPTER 179 Chiari Malformations
History
In the early 1890s, Dr. Hans Chiari, professor of pathologic anatomy at the German University in Prague, used autopsy specimens to describe four congenital anomalies later termed the Chiari malformations (types I to IV) (Table 179-1). Chiari was not the first to observe and report the type II malformations. In Observationes Medicae, written by the Dutch physician and anatomist Nicholas Tulp (1593-1674), reference is made to hindbrain herniation in a myelodysplastic individual.1 John Cleland (1835-1925) of Scotland reported a single myelodysplastic patient with hindbrain herniation and hydrocephalus in 1883. Temporally, Julius Arnold (1835-1915), professor of anatomy at Heidelberg, described a single myelodysplastic patient with hindbrain herniation and no hydrocephalus. Although the term Arnold-Chiari malformation has been used specifically in reference to hindbrain herniation in myelodysplastic patients, it was Chiari who described and attempted to delineate the pathophysiology of these posterior fossa abnormalities. As such, it is most appropriate to refer to this abnormality as the Chiari II malformation.2
TABLE 179-1 The Chiari Malformations
| CHIARI TYPE | FEATURES |
|---|---|
| I | |
| II | |
| III | High cervical or occipital encephalocele containing herniated cerebellar and brainstem tissue |
| IV | Hypoplasia or aplasia of the cerebellum and tentorium cerebelli |
Terminology
Chiari I Malformation
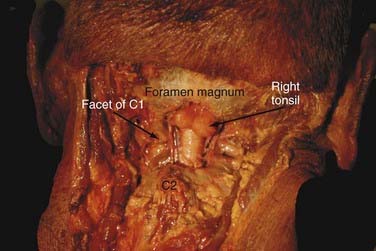
The Chiari I malformation (CIM) consists of caudal displacement of the cerebellar tonsils into the upper cervical spinal canal (Fig. 179-1). The most common associated findings are cervical syringomyelia and on occasion hydrocephalus. Multiple associations have been cited in the medical literature regarding this malformation. The full foramen magnum potentially compresses the herniated cerebellar tissue and restricts normal CSF flow across the craniocervical junction.
Chiari II Malformation
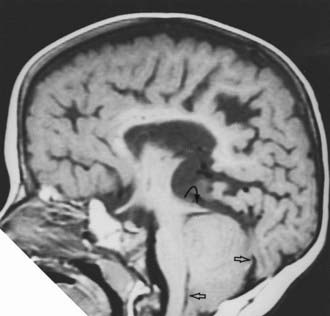
The Chiari II malformation (CIIM) is seen almost exclusively in the setting of myelodysplasia and hydrocephalus. In type II malformations, the structures herniating through the foramen magnum include the cerebellar vermis, brainstem, and fourth ventricle (Fig. 179-2). In addition to these neural structures, the accompanying choroid plexus and the associated basilar artery and posterior inferior cerebellar arteries may also be caudally displaced. The posterior fossa is often small and the foramen magnum expanded, and syringomyelia is seen in many of these patients.
Chiari III Malformation
The Chiari III malformation is the rarest of the Chiari malformations, with herniation of cerebellum and brainstem into a posterior encephalocele. This is the most severe form of hindbrain herniation, and its management is often problematic from both a technical and an ethical point of view. Lesions that prominently involve the posterior fossa contents must be distinguished from high cervical myelomeningoceles, which may look the same superficially but carry a more favorable prognosis.3,4 Patients with a Chiari III malformation generally have a poor prognosis. Severe neurological, developmental, and cranial nerve defects, in conjunction with seizures and respiratory insufficiency, are common. Surgical planning follows the same basic principles of encephalocele closure.
Chiari 0 Malformation
The Chiari 0 malformation is defined as syringomyelia without tonsillar herniation that responds to posterior fossa decompression. Iskandar and associates5 identified five patients with syringomyelia and no evidence of tonsillar herniation. MRI of the entire neuraxis ruled out other causes of a syrinx. Ultimately, abnormal CSF flow at the posterior fossa or foramen magnum was the suspected cause. All five patients underwent a posterior fossa decompression and duraplasty without direct fenestration or management of the syrinx. Significant syrinx and symptom resolution was observed in all patients. Their response to surgery suggests that “Chiari-like” pathophysiology may be present in the absence of tonsillar herniation, which may possibly be intermittent. This contention is supported by the identification of a crowded foramen magnum in two patients, multiple arachnoid adhesions in two others, and a fourth ventricular arachnoid veil in one. Each of these findings can alter CSF flow, although at present the pathophysiology resulting in syrinx formation in this group of patients is poorly understood. As such, a thorough evaluation to exclude other causes of syrinx is necessary before consideration of posterior fossa decompression.
Chiari 1.5 Malformation
Implying that only cerebellar tonsillar tissue is herniated through the foramen magnum, the Chiari I malformation (CIM) does not adequately define varieties of hindbrain herniation that also include descent of the brainstem. From our series of 130 surgical pediatric patients with CIM, we found that 17% had an additional component of brainstem descent.6,7
Signs and Symptoms
Chiari I Malformation
Patients with CIM may present with a variety of symptoms and signs ranging from headache to severe myelopathy and brainstem compromise (Table 179-2). The most common presenting symptom is pain (60% to 70%),8–10 usually occipital and upper cervical in location, and often induced by Valsalva maneuvers such as laughing, sneezing, and coughing. In infants and children who are unable to communicate verbally, headaches may manifest simply as crying and irritability. Other common symptoms include weakness or numbness, loss of temperature sensation, and unsteadiness. Careful investigation reveals that more than 70% to 80% of patients have some type of ophthalmologic or otologic disturbance at diagnosis. Ophthalmologic symptoms include blurry vision, nystagmus, extraocular muscle palsies, diplopia, and visual field deficits.11–14 Otologic complaints consist of tinnitus, fluctuating hearing loss, vertigo, and nausea. Signs at presentation have included weakness, atrophy, hyperreflexia, cape-like sensory loss, ataxia, and lower cranial nerve dysfunction. By stretching the centrally located ventral white commissure through a syrinx, pain and temperature signals cannot cross to the contralateral spinothalamic tract. The loss of pain and temperature sensation occurs only at the levels that are served by stretched spinothalamic fibers. Down-beat nystagmus is reported to be specific for lesions involving the cervicomedullary junction. Abnormal abdominal reflexes are seen in patients with associated syringomyelia. Children younger than 3 years are more likely to present with lower cranial nerve dysfunction.15 This can manifest as poor feeding, failure to thrive, recurrent aspiration pneumonia, dysphagia, choking, or stridor. A diminished gag reflex is common. Vocal cord paralysis with stridor or hoarseness may be present. An inability to maintain airway patency with lower cranial nerve dysfunction may promote sleep apnea, which may be a cause for sudden death in this group.
TABLE 179-2 Clinical Presentation of the Chiari I Malformation
| SYMPTOMS |
| CEREBELLAR SYNDROME |
| Truncal and appendicular ataxia |
| BRAINSTEM SYNDROME |
| SPINAL CORD SYNDROME |
| OTHER SIGNS |
Spinal cord dysfunction is the result of direct cord compression or syringomyelia. The incidence of syringomyelia varies between 30% and 70% in CIM. Syrinx location is typically cervical, followed by cervicothoracic. Left untreated, permanent spinal cord damage can result. Progressive scoliosis is a relatively common manifestation (30%) of CIMs when there is coexistent syringomyelia.10,16 Clinical and radiographic signs that raise the suspicion of an underlying neurological defect in a patient with scoliosis include a convexity to the left, leg or foot asymmetry, male gender or prepubertal female, and obviously, any neurological deficit.3,4,16–19 The mechanism by which a syrinx causes scoliosis is not fully understood.
Chiari II Malformations
The CIIM occurs in most (>95%) patients with myelomeningocele and is the leading cause of death in treated myelodysplastic patients today. About one third of these patients develop brainstem symptoms by 5 years of age, and in excess of one third of those die, usually of respiratory failure (Table 179-3). In fact, as many as 20% of patients with symptomatic CIIMs may present as a neurological emergency. When presenting acutely, there is dysfunction of the 9th and 10th cranial nerves, affecting respiration, swallowing, and vocal cord functions; this is often accompanied by stridor, opisthotonos, and nystagmus. Symptomatic deterioration with progressive brainstem dysfunction may be irreversible and lead to death, irrespective of the type of therapy given or the speed with which treatment is instituted.20–23 This potentially catastrophic syndrome occurs most frequently in infants younger than 2 years, particularly younger than 3 months, and has been shown to be unrelated to intracranial pressure and the size or extent of symptoms of the neural tube defect.21 Patients with symptoms who survive the high-risk period (2 to 3 months of age) may improve and become clinically stable. Especially difficult to treat are neonates who fail to initiate adequate ventilation from birth. Although suspected of having inadequate respiratory drive centers and therefore little or no potential of sustained independent ventilation, their management is associated with a poor outcome and difficult ethical decisions.
TABLE 179-3 Clinical Presentation of the Chiari II Malformation
| NEWBORNS |
| (Usually asymptomatic) |
| INFANTS |
| OLDER CHILDREN AND YOUNG ADULTS |
| NEUROLOGICAL EMERGENCY |
Unlike patients with CIM, there is a strong relationship between the type of symptoms and the age of onset. Newborns usually have symptoms. Older children and young adults most commonly display symptoms and signs of spinal cord and cerebellar dysfunction.2–424 A multitude of other symptoms and signs may occur in older patients. Common among these are ophthalmologic findings, which include strabismus, horizontal nystagmus (especially when looking upward), abnormalities of pursuit movements and convergence, and defects of optokinetic movements.25
Diagnostic Studies
Computed Tomography and Magnetic Resonance Imaging
Chiari I Malformations
The diagnosis of CIM should include the absence of an intracranial mass lesion, Dandy-Walker malformation, or hydrocephalus, all of which may cause tonsillar displacement secondary to raised intracranial pressure.26 The true incidence of CIM is not known. However, Meadows and colleagues27 found that of 22,591 patients who underwent MRI of the head, 175 (0.775%) were found to have tonsillar herniation extending more than 5 mm below the foramen magnum.
The position of the cerebellar tonsils in the normal population was studied by Aboulezz and colleagues.28 In a review of 800 MRI examinations, the authors noted that normal or asymptomatic patients may have tonsils that extend 3 mm below the foramen magnum. The tonsillar herniation was noted to be clearly pathologic when it exceeded 5 mm and borderline between 3 and 5 mm. Similarly, Barkovich and colleagues29 studied 200 normal patients and 25 patients with a “firm” diagnosis of CIM. The authors concluded that, in the absence of syringomyelia, 2 mm of tonsillar ectopia was of minimal clinical significance. Recently, Mikulis and associates30 determined that age affects the normal position of the cerebellar tonsils, with ascent of the tonsils with increasing age.
Other associated radiologic anomalies occur infrequently and include most commonly atlanto-occipital assimilation, platybasia, basilar invagination, and fused cervical vertebrae.26 Despite the less frequent occurrence, these changes should be sought because they can lead to cervical instability.
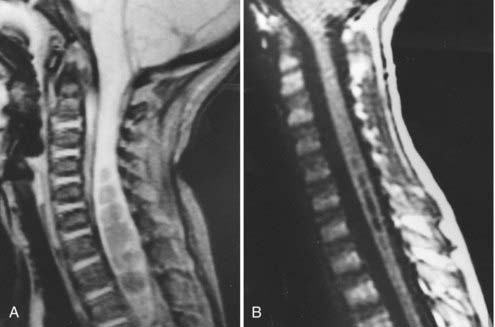
In addition to the absolute position of the tonsillar tips, the configuration of the tonsil is important. The tonsillar tip may be pointed and drawn out and may carry more pathologic significance, or it may be blunt and rounded and be less concerning. Syringomyelia occurs commonly with CIMs and can be seen in 50% to 70% of patients (Fig. 179-3).
Chiari II Malformations
CIIMs are characterized by the elongation and caudal displacement of the cerebellar vermis and brainstem, the presence of a myelomeningocele in virtually all cases and hydrocephalus in most, and the common (40% to 95%) existence of syringomyelia, especially in the lower cervical cord. However, the changes of the CIIM constitute a set of cranial and spinal malformations ranging from the posterior fossa, upper cervical canal, ventricular system, and neural tissues of the brain.31–37
Associated neurological anomalies include tectal beaking, secondary to partial or complete fusion of the colliculi into a single backward pointed peak, and kinking at the level of the cervicomedullary junction (Fig. 179-4). The latter anomaly is caused by caudal displacement of a portion of the medulla in conjunction with a spinal cord that is held in relative immobility by the dentate ligament. The cerebellum is smaller than usual, and upward herniation of the cerebellum may be evident. Finally, callosal agenesis or dysgenesis, as well as abnormalities of the cerebral cortical pattern termed polygyria (not to be confused with the abnormal four-layered cortex seen in polymicrogyria) have frequently been described in Chiari II patients.34

In addition to hydrocephalus, the ventricular system displays multiple abnormalities. The third ventricle may be only mildly dilated and contains a large massa intermedia. The fourth ventricle is typically small or nonvisualized and often flattened and elongated, and it extends into the cervical canal. The lateral ventricles may be asymmetrically dilated, with prominence of the atria and occipital horns (colpocephaly), and the septum pellucidum is frequently absent. This sharpness of the frontal horn (lemon sign) and the caudal displacement of the fourth ventricle (banana sign) are relatively easily seen on in utero ultrasound examinations.38,39
The upper cervical canal also displays several bony and spinal cord anomalies in association with the CIIM. The posterior C1 arch is often missing. Klippel-Feil fusion anomalies of the cervical spine are present in a small group of patients. Basilar impression and C1 assimilation are uncommon in CIIM. Significant shortening and scalloping of the clivus can be seen.40 Other radiographic signs of CIIM include Lückenschädel, scalloping of the posterior surface of the petrous pyramid, falx hypoplasia, falx fenestration, tentorial hypoplasia with a wide incisura and tiny posterior fossa, and enlargement of the foramen.35,36
Cerebrospinal Fluid Flow Studies and Cine-Mode Magnetic Resonance Imaging
One technique to assist in the surgical decision making of patients with Chiari malformations is motion-sensitive MRI, or cine-mode MRI. As opposed to static MRI scanning, cine MRI41–44 may demonstrate lack of CSF flow patterns that can occur in the setting of CIM. The presence of a CIM and a syrinx resulting from disturbed CSF flow, which can be demonstrated by this technique, adds helpful information to the clinical assessment.45 Repeating the study postoperatively may help in evaluating the adequacy of the decompression. Having said this, we find cine MRI of minimal utility in clinical practice and especially in patient selection for operation.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


