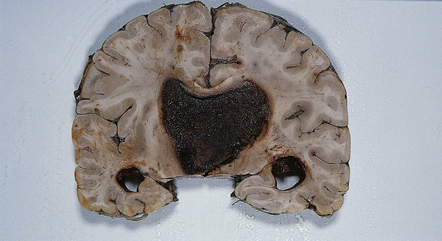
40 CPPs are well-circumscribed neoplasms with a stippled surface that reflects their papillary structure (Fig. 40.1). In contrast, CPCs tend to invade local structures. Both types of neoplasm can be highly vascular, and CPCs frequently contain foci of hemorrhage (Fig. 40.2). 40.1 CPP. CPPs resemble normal CP, being characterized by a columnar epithelium that rests on a delicate fibrovascular network and forms multiple papillary projections (Figs 40.3, 40.4). However, CPPs can be distinguished from CP because they demonstrate minor atypical cytologic features, such as: 40.3 CPP. 40.4 CPP.
Choroid plexus neoplasms
CHOROID PLEXUS NEOPLASMS
MACROSCOPIC APPEARANCES
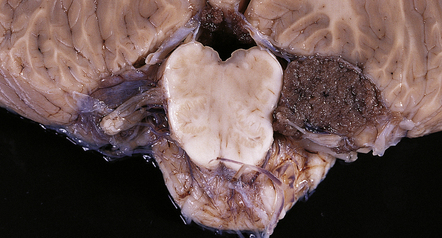
The cerebellopontine angle is an unusual site for a CPP; nearly all are intraventricular. A stippled surface resembling that of a cauliflower is evident.
MICROSCOPIC APPEARANCES
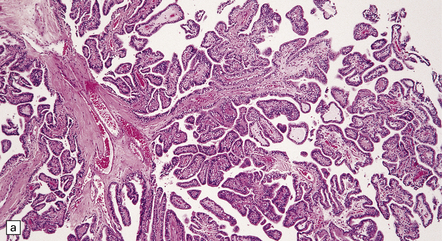
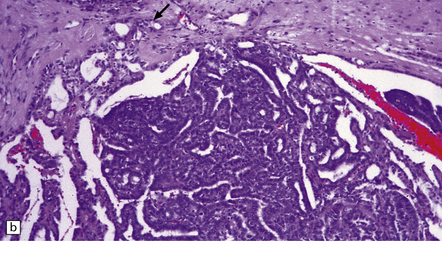
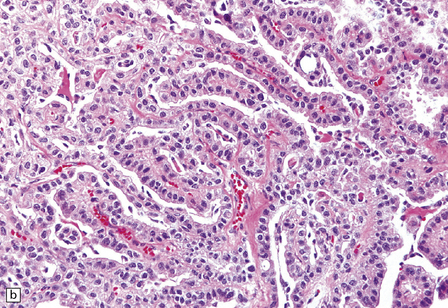
(a) In many areas, an obvious papillary architecture is found. A more complex pattern may be present in atypical CPPs (b) but this and superficial invasion of the stroma (arrow) do not warrant a diagnosis of CPC.
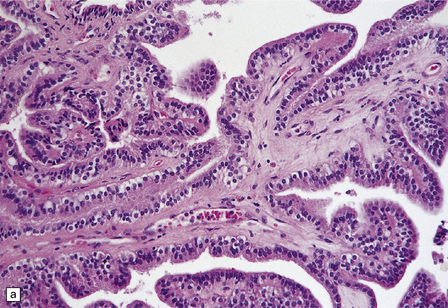
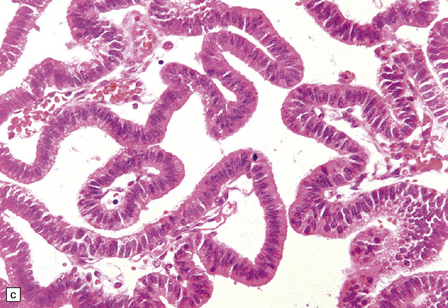
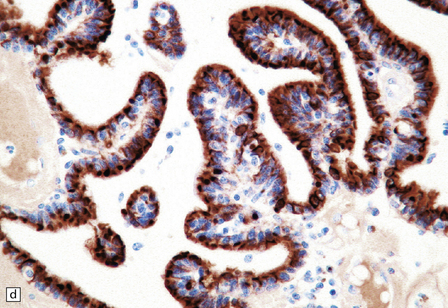
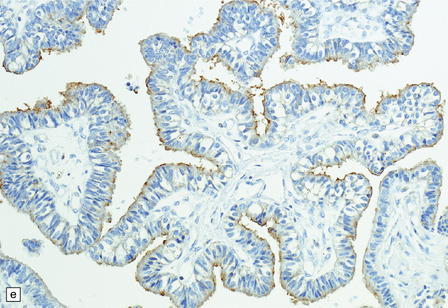
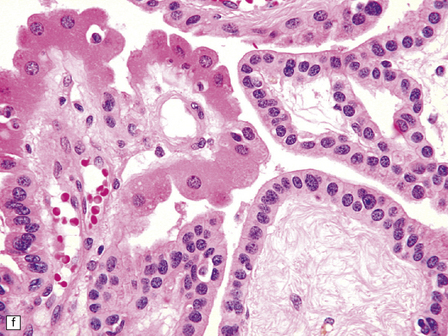
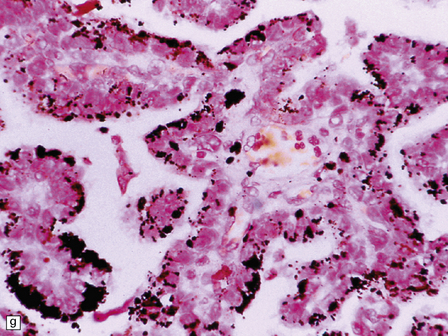
(a) A layer of cuboidal or columnar cells rests on a fibrovascular stroma. (b,c) In addition to architectural abnormalities, mild cytological atypia and occasional mitoses distinguish the CPP from CP. (d) Immunoreactivity for cytokeratins is a feature of CP tumors. (e) Kir7.1 antibodies label the membrane of epithelial cells in CP neoplasms. (f) Rare CPPs contain oncocytic cells, or (g) melanin.![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Choroid plexus neoplasms
 CHOROID PLEXUS NEOPLASMS
CHOROID PLEXUS NEOPLASMS




 GENETIC FACTORS AND CP NEOPLASMS
GENETIC FACTORS AND CP NEOPLASMS



Only gold members can continue reading. Log In or Register to continue


