Chapter 118 Cingulotomy for Intractable Psychiatric Illness
Historical Developments
For millennia, physicians have attempted to treat diseases of the mind with surgery1–7 initially in the form of cranial trepanations. In the modern era, psychiatric neurosurgery was first proposed by the Portuguese neurologist, Egas Moniz.8 Initially, Moniz injected alcohol into the white matter of the frontal lobes of institutionalized patients and while this early experience received only cautious support, the concept of a surgical therapy for psychiatric patients was rapidly adopted, culminating in Moniz being awarded the Nobel Prize for Medicine in 1949. One of the most enthusiastic proponents of this new therapy was Walter Freeman9 in the United States, who championed prefrontal lobotomy. At first his technique involved bilateral coronal sectioning of the frontal lobes via burr holes and later by a transorbital approach. These early surgical techniques were crude and associated with major morbidity and mortality as high as 10%. Complications included severe cognitive impairment, personality changes, intracranial hemorrhage, and seizures.10 The patients were believed to be “no longer distressed by their mental conflicts but also seem to have little capacity for any emotional experience.” Standard intelligence quotient (IQ) tests, however, revealed no significant postoperative deficits, and Freeman along with other practitioners at the time considered the side effects acceptable.
Surgery for intractable psychiatric illness thus became widely accepted and was used for a variety of diagnoses, including major depression, obsessive compulsive disorder (OCD), and schizophrenia. Between 1942 and 1954, more than 10,000 cases in England and Wales and more than 18,000 cases in the United States were performed.10 However, there was much controversy among neurologists, neurosurgeons, and psychiatrists who had reservations regarding the scientific, ethical, and technical aspects of psychosurgery. This controversy prompted more rigorous clinical trials with a goal to reduce lesion size to more anatomically specific brain regions.
Stereotactic neurosurgical techniques were introduced in 1947, to create accurate lesions in cortical and subcortical structures, and numerous target areas were identified, including the cingulate cortex. The methodical study of the cingulate cortex in primates was pioneered by John Fulton.11 Fulton12 was the first to suggest that the anterior cingulum would be an appropriate target for psychiatric neurosurgical intervention, and cingulotomy was initially carried out as an open procedure.13,14 Whitty in 1955 described 35 such patients of open cingulectomy,15 with most of the surgery being carried out by the late Sir Hugh Cairns of Oxford. Patients were selected based on predominant symptoms of either anxiety or obsessive behavior. The procedures were successful on the whole, with the outcome described as a “slight loss of inhibition and a reduction in tension and in the persistence of emotional and cognitive activity.”15 Foltz and White16 reported their experience with stereotactic cingulotomy for intractable pain, and noted that optimal results were achieved in patients with concurrent anxiety-depressive states. Ballantine and colleagues17 subsequently demonstrated the safety and effectiveness of cingulotomy in a large number of patients, and it has been the surgical procedure of choice in North America over the last 3 decades. In Europe, alternative targets were being used, such as subcaudate tractotomy,18 anterior capsulotomy, and limbic leucotomy (a combination of cingulotomy and subcaudate tractotomy).19
Concurrent to the development of stereotactic surgical techniques and safer more discrete lesions, psychotropic drugs were introduced that offered a safe alternative therapy and new hope. Chlorpromazine became available for use in the United States as an antipsychotic in 1954, and approval of major antidepressant medications soon followed. Pharmacotherapy was rapidly embraced by the psychiatric community, and consequently there was a dramatic decrease in the demand for surgical intervention. Currently the accepted therapeutic approach to most psychiatric disease involves a combination of psychotherapy, pharmacotherapy, and electroconvulsive therapy. Despite these modern treatment methods, many patients fail to respond adequately and remain severely disabled. In these patients, surgical intervention may still be considered appropriate if the therapeutic result and overall level of functioning are improved. Although our understanding of the anatomy and physiology of surgical lesions has improved and our ability to place discrete and accurate lesions in targets of interest has progressed, the debate and controversy in this area continue.
Functional Neuroanatomic Basis for Cingulotomy
The cingulate (from the Latin for belt) gyrus lies on the medial surface of each cerebral hemisphere adjacent to the falx cerebri and forms part of the “limbic lobe.” The underlying subcortical white matter, the cingulum bundle, connects the cingulate gray matter with various regions, including prefrontal cortical areas, basal ganglia, thalamus, and mesial temporal structures, as well as connecting the anterior perforated substance with the parahippocampal gyrus.7,20,21 Histologically, the cingulate cortex consists of mesocortex and a transitional cortical architecture between the six-layer neocortex and the three-layer paleocortex.22 Based on function and architecture, the cingulate cortex is often divided into an anterior and posterior division. The anterior division is involved in executive functions, whilst the posterior part is sensory and limbic related. The anterior cingulate may be further subdivided into dorsal and ventral parts, involved in cognitive and affective functions respectively.
In 1937, Papez23 published “A Proposed Mechanism of Emotion,” in which he postulated that a reverberating circuit in the brain might be responsible for emotion, anxiety, and memory. The anatomic components of this circuit consisted of the hypothalamus, septal area, hippocampus, mammillary bodies, anterior thalamic nuclei, cingulate gyri, and their interconnections. This rudimentary limbic system was subsequently expanded to include paralimbic structures, including orbitofrontal, insular and anterior temporal cortices, the amygdala, and dorsomedial thalamic nuclei.24 The hypothalamus, a central component in this system, controls autonomic function, and these functions in humans are often accompanied by subjective experiences and behavioral patterns. Stimulation of the hypothalamus in animals produces autonomic, endocrine, and complex motor effects, which supports the idea that the hypothalamus integrates and coordinates the behavioral expression of emotional states.25 The neural outflow from the hypothalamus can be modulated by cortical and brainstem inputs, and the limbic system represents a direct pathway to the hypothalamus. Neocortical areas are connected to the limbic system proper by paralimbic structures.26 The limbic system appears to interconnect visceral and somatic stimuli with higher cortical functions and in this way may “add an emotional component to the psychic process.”23
Although the exact neuroanatomic and neurochemical basis of emotion in health and disease remains undefined, there is evidence that the limbic system and its interconnections with the basal ganglia and forebrain play a central role in the pathophysiology of psychiatric disorders. Electrical stimulation of specific areas within the limbic system (i.e., the anterior cingulate) has been shown in humans to alter autonomic responses and anxiety levels27,28 and can cause movements in awake patients that resemble compulsive actions.29 Neuroimaging studies also implicate a circuit composed of orbitofrontal cortex, striatum, thalamus, and anterior cingulate cortex in the pathophysiology of OCD. Abnormalities of glucose metabolism have been found in the caudate nucleus, orbitofrontal cortex, and cingulum in patients with OCD on positron emission tomography (PET).30,31 Specialized PET images taken of patients during obsessive states reveal uniform hypermetabolism in the caudate nucleus, anterior cingulum, midfrontal cortex, and left thalamus, all structures connected with the limbic system.32 Similarly, PET studies have shown that reduced glucose metabolism in the lateral frontal cortex is a correlate of the depressive state in certain patients.33
The cortical-striatal-pallido-thalamic connections that have been well characterized for the control of motor function may explain some features of OCD. Modell et al.34 proposed that this network consists of two components: an orbitofrontal-thalamic loop mediated by the excitatory neurotransmitter glutamate and an orbitofrontal-striatal-thalamic loop mediated by various transmitters, including glutamate, dopamine, serotonin, γ-aminobutyric acid, and glutamate. With this model, overactivity of the orbitofrontal-thalamic loop results in obsessive compulsive behavior. Neurochemical models suggest that affective and anxiety disorders may be mediated via monoaminergic systems. In particular, the serotoninergic system has received emphasis with respect to OCD. Because of the diffuse nature of the monoaminergic projections and their role as neuromodulators, however, these models are not particularly instructive in terms of the functional neuroanatomy relevant to different neurosurgical treatments as they are currently used.
Although the exact neuroanatomical and neurochemical mechanisms underlying depression, OCD, and other anxiety disorders remain unclear, it is appealing to believe that these psychiatric disorders might reflect a final common pathway of limbic dysregulation, which can be modulated surgically. Neurobiological models of anxiety and affective disorders have also emphasized the fundamental role of the limbic system and its related structures.34–36 Almost all psychosurgical procedures have been directed at some component within this system, giving rise to the less emotive term of limbic system surgery.
Indications
Cingulotomy has been performed successfully for a number of psychiatric disorders including major affective disorders, obsessive compulsive disorder, addiction, as well as chronic pain. Patients considered for cingulotomy should have demonstrated a severe, chronic, disabling, and treatment-refractory psychiatric illness. Illness severity should be manifest in terms of subjective distress and a decrement in psychosocial functioning. Chronicity refers to the enduring nature of the illness and in some cases may be less important than severity. The illness must also be refractory to systematic trials of pharmacologic, psychological, and, when appropriate, electroconvulsive therapy before considering neurosurgical intervention.
The major psychiatric diagnostic groups that might benefit from cingulotomy are1 chronic anxiety states, including OCD, and2 major affective disorder (i.e., major depression or bipolar disorder). Patients who present with mixed disorders demonstrating a combination of symptomatology of anxiety, depression, and OCD, may still be candidates for psychosurgery. Schizophrenia is currently not considered an indication for cingulotomy. Relative contraindications include a history of a significant personality disorder, other axis II symptoms substance abuse, or acute suicidality. Patient selection is probably the single most important issue in psychiatric surgery, and although the patient undergoes a multidisciplinary review, the responsibility of selection for surgery rests with the psychiatrist, who may also be responsible for long-term postsurgical management.
Surgical Technique
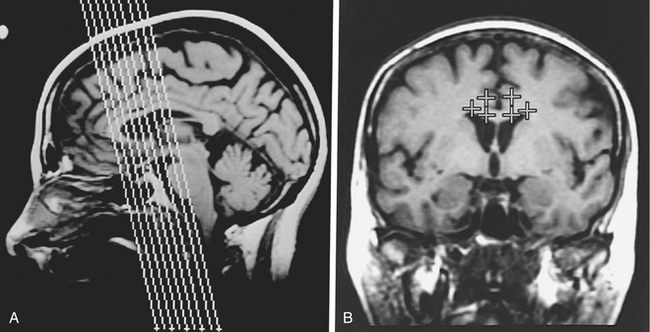
Briefly, an MR stereotactic compatible frame is fixed to the patient’s cranial vault under intravenous sedation and after infiltration of the pin insertion sites with local anesthesia. Oblique coronal MR images are then obtained and typically, target coordinates are calculated for a point in the anterior cingulate gyrus 2 to 2.5 cm posterior to the tip of the frontal horn, 7 mm from the midline, and 2 to 3 mm above the corpus callosum bilaterally (Fig. 118-1).
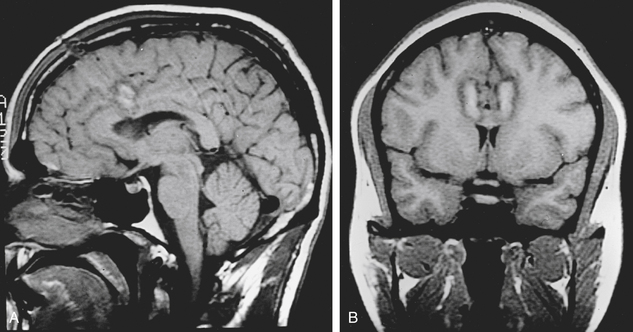
After the target coordinates are calculated, the trajectory is optimized and entry point noted. The patient is positioned on the operating table and the stereotactic frame is secured to the table. A supine or semireclining position on the operating table is suitable with the head positioned low enough to prevent air embolism. Under local anesthesia, the skin is then incised. A variety of skin incisions may be chosen, such as bilateral 1-cm straight incisions or a bicoronal skin incision. Intracranial access is gained via bilateral burr holes with a perforator 15 to 25 mm from the midline. In general, a handheld drill is preferred to a pneumatic-powered drill to minimize patient anxiety. The dura is opened and an entry point chosen to avoid cortical vessels. A standard thermocoagulation electrode (Radionics, Inc., Burlington, MA) with a 10-mm uninsulated tip is inserted to the target and heated to 85°C for 90 seconds. After adequate cooling, the electrode is then withdrawn 5 to 10 mm, and a second lesion is made, using the same lesion parameters to ensure complete ablation of the cingulate gyrus. This results in a lesion of approximately 1 to 2 cm in vertical height and 8 to 10 mm in diameter in the anterior cingulum (Fig. 118-2). The procedure is then performed in an identical fashion on the opposite side.
< div class='tao-gold-member'>
Related posts:
 Cortical and Subcortical Brain Mapping
Cortical and Subcortical Brain Mapping
 Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
 Surgical Management of Tumors of the Foramen Magnum
Surgical Management of Tumors of the Foramen Magnum
 Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
 Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
 Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


