and Colin L. W. Driscoll2
(1)
Department of Otolaryngology – Head and Neck Surgery, Stanford University, Stanford, CA, USA
(2)
Department of Otorhinolaryngology, Mayo Medical School, Rochester, MN, USA
Concept
The approach combines a presigmoid, retrolabyrinthine craniotomy with a middle fossa craniotomy.
The two craniotomies are connected by splitting the superior petrosal sinus and dividing the tentorium.
Conditions treated
Petroclival meningiomas
Trigeminal schwannomas
Epidermoids of the cerebellopontine angle and ventral pons
Other lesions that extend into both the middle and posterior fossa
Risks
Labyrinthine injury with hearing loss and dizziness
Facial nerve injury
Palsy of CN III, IV, VI
Damage to the vein of Labbé, which could produce temporal lobe infarction
Seizure
CSF leak
Benefits
Excellent exposure of the posterior fossa and middle fossa is provided. The view extends from the posterior communicating artery within the Circle of Willis and CN III superiorly to the jugular foramen and CN XI inferiorly.
Hearing, balance, and facial nerve function can be preserved.
1.
Overview of the bone to be removed (gray). Additional bone can be removed posterior to the sigmoid sinus to allow for greater retraction and exposure in the posterior fossa. This additional exposure also improves the trajectory to the internal auditory canal, jugular bulb, and petrous apex as viewed posteriorly. It helps with seeing “around” the intact semicircular canals to address tumor in the temporal bone.
2.
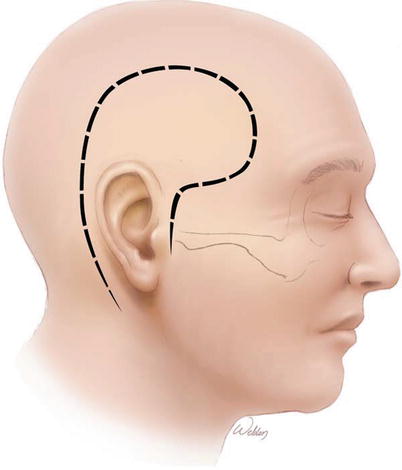
The incision is marked so as to course around the temporalis muscle boundaries yet still end up in the preauricular crease to reduce visible scarring and prevent injury to the frontal branch of the facial nerve. For tumors that do not extend far anteriorly in the middle fossa, it can be adequate to omit the descending part of the anterior limb of the incision.
3.
The superficial tissues are elevated off the mastoid and temporalis muscle and retracted anteriorly and inferiorly. The ear canal tethers this tissue, and it is important not to tear into it and contaminate the sterile field.
4.
The temporalis muscle is then elevated and retracted anteriorly. If desired, it could be left attached to the skin flap and the entire mass of tissue elevated off the skull at once.
5.
A mastoidectomy with sigmoid sinus decompression is performed. The middle fossa and posterior fossa dura is exposed. The additus ad antrum is seen but not widely opened as it will have to be sealed off at the end of the procedure to prevent CSF leak. These steps are exactly the same as the initial steps in the translabyrinthine approach. One difference is that all three semicircular canals must be clearly delineated and the bone around them thinned. The canals do not need to be “blue lined,” but every millimeter of bone removal is critical for achieving excellent exposure.
6.
The temporal lobe dura is dissected away from the inner surface of the skull with a Penfield elevator and a craniotome then used to turn a bone flap in one piece.
For tumors that do not involve the temporal bone such as a bilobed trigeminal nerve schwannoma, this amount of temporal bone removal will provide acceptable exposure. Some tumors will also have significant extension into or involvement of the temporal bone, particularly chondrosarcomas and many meningiomas. In these cases, one can perform the middle fossa craniotomy and then remove bone in the petrous apex, even identifying and skeletonizing the internal auditory canal. Similarly, one can work around the endolymphatic sac/duct, removing bone deep into the petrous apex in the retrofacial and retrolabyrinthine areas when needed. Some meningiomas and epidermoids may have tumor extension in the internal auditory canal that can be exposed in this manner. In both situations, removing the tumor in the temporal bone prior to opening the dura has the added advantage of decreasing the vascular supply of the remaining tumor.
Achieving adequate retrofacial/retrolabyrinthine exposure to visualize the internal auditory canal often requires more bone removal posterior to the sigmoid sinus to have the proper view. Some advocate removing the posterior semicircular canal and occluding with bone wax to gain added access. While hearing might be preserved, it is certainly put at increased risk, and we have not found it to be necessary.
7.
The dural incisions are shown. For optimal exposure, the inferior limb of the incision needs to go all the way down to the sigmoid “crotch” (arrow). This is the region where the sigmoid sinus curves around to rise up to the jugular bulb. Also, the dural opening should cross the superior petrosal sinus midway between the transverse-sigmoid junction and the petrous apex bone (arrowhead). Dividing this too far posteriorly may impact temporal lobe venous drainage, particularly if the vein of Labbé joins with the superior petrosal sinus, a frequent anatomic variant.
8.
Typically, the posterior fossa opening is performed first to release CSF. The middle fossa opening is then performed. Retractors are used on top of moistened Telfa strips to protect the brain. Importantly, the vein of Labbé should be identified prior to connecting the two dural openings (See Chap. 8, images 98 & 99 for an example of how to identify the vein of Labbé). It is critical to not inadvertently transect it while opening the dura around the superior petrosal sinus. Once the vein of Labbé has been protected, the superior petrosal sinus can be either cauterized with a bipolar or clipped prior to transaction. The remaining dural incision can then be safely performed.
Following this, the tentorium is divided. There are veins within the tentorium, particularly medially and anteriorly, that anastomose with the cavernous sinus. Thus, the tentorium should be incised in a stepwise fashion by first cauterizing a section with a bipolar and then cutting that section with a scissors.
When nearing the tentorial notch, CN IV (arrow) should be identified within the surrounding arachnoid and dissected free of the tentorium so it is not damaged when cutting the tentorium. It is usually superior to the notch slightly but may also be found inferior to it occasionally.
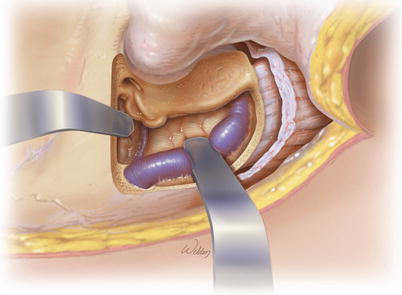
9.
After dividing the tentorium, the retractors work much more effectively, and visualization of the petroclival junction is substantially enhanced. This illustration indicates all the structures that can be seen after the opening has been completed. However, in reality, these structures cannot all be seen simultaneously as shown. The microscope will need to be positioned at different viewing angles to see them all.