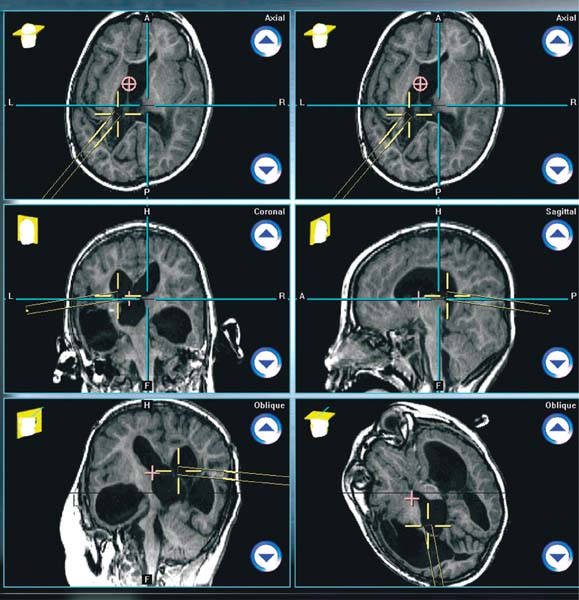
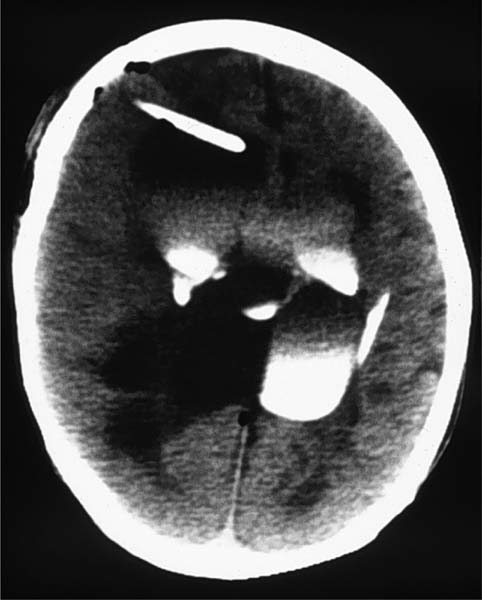
4 Compartmentalized Hydrocephalus Compartmentalized hydrocephalus, also referred to as multiloculated or multicystic hydrocephalus, is a known and dreaded complication of an inflammatory process within the cerebrospinal fluid (CSF) compartments of the brain. Although rare, when present it significantly increases the complexity in treating the associated hydrocephalus. Until the reintroduction of the endoscope to neurosurgeons in the mid-1980s, the two treatments available were multiple shunt catheters and craniotomy. As neuro-surgeons have become more facile with endoscopy, the management of this condition has increasingly been dependent on fenestration of these spaces endoscopically. What follows is a discussion of this entity, its management with the endoscope, the complications seen, and the outcome. Fluid spaces can become trapped or isolated in response to an inflammatory process within the CSF compartments of the brain. The most common sources for this process, or ventriculitis, are infection and hemorrhage.1–3 Small passageways between the ventricles, such as the foramina of Monro, Magendie, and Luschka, and the sylvian aqueduct can scar over, entrapping the upstream ventricular space (s). Additionally, hemorrhage within the germinal matrix of a premature infant or a severe infectious ventriculitis, such as is seen with gram-negative or fungal organisms, can cause the subependymal layers to dissociate from adjacent parenchyma, thus giving rise to one or more sequestered spaces that grow into the adjacent ventricle. Further complicating this process is that over time this dissociative process can evolve, leading to new cysts forming months after the offending force has been dealt with.4 Finally, an infection that is extremely pyogenic will create a turbid CSF that will result in an extremely inflamed ependyma, which will scar when in contact with adjacent ependymal surfaces, leading to entrapped CSF spaces. The end result of the processes described above is one or more CSF spaces that are no longer in communication with the normal CSF circulatory pathways or that are no longer in communication with a shunted CSF space. These trapped spaces can accumulate fluid over time either from choroid plexus residing within the trapped space or from transudate from the walls of the space. As the fluid accumulates, the size of the space increases, and it becomes a mass that causes the intracranial pressure to rise. It is at that point that the patient begins to deteriorate clinically. Fenestration of multiple intraventricular cysts has come to be favored over the use of catheters. Managing a ventricular drainage system that incorporates multiple proximal catheters can be complicated, and when such a system is used to drain multiple subependymal cysts, there is a tendency for the cysts to collapse down around the catheters and occlude them. Before endoscopy became widely available, managing such a patient usually ended in craniotomy to fenestrate the cysts into one large fluid space after multiple trips to the operating room for addition and revision of proximal catheters.5 Consequently, neurosurgeons welcomed the addition of the endoscope to their armamentarium. Their excitement, however, was soon blunted when they realized that these cysts typically lacked landmarks. Only with the addition of image guidance systems did the endoscope become a truly effective tool for managing multiloculated ventricles. Over the past several decades, there has been a tremendous advance in the use of neuroendoscopy for managing various intraventricular pathologies, including multiloculated ventricles. This is due to improvements in the optics of the endoscope, improved imaging technology, and the marriage of image-guided surgery with neuroendoscopy.6Also important has been the development of instruments such as microforceps, lasers, saline torches, and microballoons.7–11 With these advancements have come increasing reports of their use for fenestration of septations within hydrocephalic ventricles or the septum pellucidum in isolated ventricles, fenestration of arachnoid cysts and tumor cysts such as seen with craniopharyngioma, and placement of catheters in ventricles or intratumor cystic cavities. Of these it could be argued that the management of multiloculated ventricles has experienced the greatest change due to the introduction of the endoscope. In approaching multiloculated ventricles with the endoscope, the surgeon should first consider the type of scope to use. Available are fiberoptic scopes with deflec-table tips, semirigid or rigid fiberoptic scopes, and rigid glass rod or lens scopes. The advantage of a rigid lens scope is the superior visualization of structures that it provides. The image that this system projects to the camera is a perfect reflection of the surgical field, and it can be magnified to infinity with crystal clarity. The disadvantage of this type of scope is that, because it is a rod, its tip cannot be deflected to inspect a wider field of view. The view can be widened only by changing the scope to another with a different angulation in its tip’s lens (e.g., exchanging a 0-degree scope for a 30-degree scope to see the margins of the field better). Flexible fiberoptic scopes with deflectable tips will allow for greater fields of view, but the conduction of the image from the tip to the camera degrades the image quality, resulting in a poorer image as compared with a lens scope (so-called pixilation). Semirigid or rigid fiberoptic scopes’ main advantage is their size; they suffer the same disadvantage as flexible fiberoptic endoscopes. One option for the surgeon is to use both a rigid lens scope and a flexible fiberoptic scope to manage multiloculated ventricles, as advocated by Oi.12 The superior image of the rod scope can be used to familiarize the surgeon with the anatomy present, and the flexible scope can be used to better navigate the environment to accomplish the surgical goals. There is a growing list of instruments available to the endoscopist to manage multiloculated ventricles. For fenestration, there are monopolar and bipolar cautery units, as well as lasers. Fogarty catheters or specially developed microballoons can be used for enlargement of small fenestrations. Tissue can be cut with specialty knives or scissors that fit the endoscope’s working channels, and tissue can be removed with various types of forceps that work with the endoscope. Increasingly sophisticated holding devices for endoscopes have been developed; some even include micro-manipulators that allow for precise, small movements of the scope once on site in the surgical field.6 The use of these devices is somewhat controversial in that they limit large movements of the scope, tending to confine the surgeon’s field of interest. An important aspect of multiloculated ventricles is that normal anatomical landmarks are frequently masked or absent. Consequently, targeting a fenestration can be difficult. The introduction of intraoperative ultrasound and image-guided surgery has been an effective answer to this problem. A second bur hole will allow for the use of ultrasonography during an endoscopic procedure. The ultrasound can be used to visualize the turbulence of irrigation as it leaves the tip of the endoscope, allowing the endoscopist to understand just where in the fluid space the scope’s tip is.13 The difficulty with this technique, however, is that the image is two dimensional, and the ultrasonic head must be rotated to see the scope’s tip in a different plane. If the jet of fluid emerging from the tip is not parallel to the image’s plane, it will not be seen. Image guidance is a better answer for the orientation problem. For rigid scopes, tracking devices can be affixed to the scope, allowing tracking of the tip during the surgery (Fig. 4.1). When projected onto preoperative imagery, targeting of the fenestrations becomes very straightforward. If flexible scopes are to be used, a tracking device can be attached to the channel through which the scope will be delivered to the target. Tracking probes can be used as obturators for the scope’s channel to orient the placement of the channel at the intended fenestration site. Potentially, all the instruments mentioned above may be needed during the procedure, so steps should be taken to ensure they are compatible with the scopes planned for use. Assisting personnel should be familiar with the instrumentation to be used and how to troubleshoot any problems. They should also be aware of the flow of the case and anticipate the surgeon’s needs during the operation. This is critical in endoscopy, as the surgeon is commonly working in tight spaces near critical structures. Time on site should be kept to a minimum to avoid surgeon fatigue that will occur as a result of controlling the scope in such an environment. It is not a bad idea to rehearse the surgery mentally or at least to go through the steps of the procedure in advance with the assisting personnel. The surgeon should be familiar with his or her instrumentation, their capabilities, and their appropriateness for the demands that will be present during the procedure. He or she should also be aware of what backup equipment is available, how to use it, and where it is located. It is useful to spend some time studying the patient’s radiographs. First, goals for the surgery are set. When multiple cysts are present, it may be impossible to fenestrate them all through a single bur hole. As the cysts are fenestrated and the CSF drained, there will be an expected shift in the anatomy, making the preoperative films irrelevant. Thought should be given to the anatomy underlying the walls of a fluid space that is being fenestrated, particularly if that space is narrow. The planned surgery should occur along a straight line, as it is much simpler to stay oriented in this situation than it is when multiple turns must be taken. Computer-assisted navigational equipment can be useful for this by establishing a line of targeted cysts and points for their fenestration, then drawing the line out to the skull’s edge to locate the bur hole. Also, by studying the anatomy as seen on the image set, the surgeon can anticipate where visible landmarks might be that will help with orientation during the procedure. Finally, it is important during planning to acknowledge that in many cases all the cysts cannot be fenestrated in a single setting. There is nothing wrong with sharing this with the patient’s family and telling them that instead of one large craniotomy, several relatively minor surgeries may be needed. Postoperative imagery can be used to determine what has been accomplished and what is left to fenestrate. A postoperative computed tomography (CT) scan with contrast injected into the ventricles to determine what has been communicated can be very helpful in this regard (Fig. 4.2). Fig. 4.1 Endoscope’s guide sleeve being tracked as it moves to the target. Fig. 4.2 Contrast injection via a shunt into the ventricles showing which have been successfully communicated. Once a surgical plan has been made, the patient is brought to the operating room. Ideally, the patient should be positioned in such a manner that the planned bur hole will be at the apex of the surgical field. This will minimize loss of CSF during the procedure. Sometimes this can be difficult, though, as another requirement of patient positioning is the need to reference to the guidance system. With careful planning and forethought, these two goals can be accomplished. After drilling the bur hole, the guidance system is used to place the endoscope’s working sleeve at the first fenestration target. The system can be used for placement at other fenestration targets, but it must be remembered that the accuracy of the guidance system degrades with fenestration of cysts that are under pressure and the loss of CSF. With each fenestration the surgeon should become increasingly conservative and more reliant on landmarks in the operative field. If there are no landmarks, and the surgeon is concerned about shifting anatomy, then the procedure should be stopped and postoperative imagery obtained to assess what remains to be done.
Endoscopic Fenestration
Pathophysiology
Treatment
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


