10 Disorders of sensation and perception
At the end of this chapter, you should be able to:
• detail the processes involved in sensation, and compare and contrast these with perception
• explain the terms bottom-up, top-down and network processing, and apply these to human perception
• explain how a neurological condition could impact on sensation and perception, and give rise to perceptual disorders
• define the concept of pain, describe the processes involved in pain perception, and explain how a neurological condition, such as stroke, may impact on this
• detail some of the difficulties associated with the assessment of pain in people with neurological conditions.
Introduction
The senses that we possess (sight, hearing, touch, taste, smell and proprioception) are used by us all continuously throughout each day of our life. Their apparently flawless function makes that their essential contribution to our existence is rarely appreciated. Consider the example where, in your university cafeteria, you have made your selection of food and drink and placed this on your tray. Joining the queue at the cash till, you meet one of your lecturers. You engage in a lively debate about the lecture you just had, while balancing your tray on which there is a bowl, filled to the brim, with hot soup. Although the balancing is a seemingly effortless task, the fact that you perform it without conscious awareness does not render this a simple problem. While conducting your conversation your proprioceptors – the sensors in your muscles, tendons and joint capsules that provide information about your posture and movement – as well as various sensors in your skin, continuously detect changes in joint position and orientation, speed, pressure and shear forces in your skin. This afferent information is relayed to the spinal cord, where it feeds into various reflex loops under higher cortical and cerebellar influence (Chapter 6). The resulting motor output is geared towards maintaining a level position of your tray to ensure your soup does not spill over and create a mess, as well as preserve your posture.
People with the – albeit rare – condition of sensory neuropathy would probably not be able to do this; they would be unable to feel the position of themselves – or the tray – in space. With afferent information being corrupted or lacking altogether, the postural reflex mechanisms are unable to produce the required output, and the person would be likely to drop the tray. A fascinating study can be found in Sacks (1985), where he describes the case of a so-called ‘disembodied lady’. Bereft of proprioception due to a rare infection, she does not ‘feel’ her body, and lacks the unconscious control to stabilise her posture. Through the process of rehabilitation, she learns to compensate for the lack of automatic posture control by using vision, and by consciously focusing her attention, e.g. by looking at her tray. But the moment her attention is distracted and she looks elsewhere, her posture collapses. Such profound isolated impairments of proprioception are rare; however, case studies such as this highlight the important role of sensory information in our daily activities and illustrate how senses can compensate for each other to a certain degree.
The aim of this chapter is to compare and contrast ‘sensation’ with ‘perception’, detail the various stages involved in information processing, and explain the impact that a neurological condition, e.g. stroke, may have on this. We will focus on pain perception in particular, as an analysis of this phenomenon demonstrates how sensation, perception, as well as cognition interact in creating this unpleasant experience. Studying the process of ‘central post-stroke pain’ also helps to deepen our understanding of the impact that a lesion of the central nervous system may have on signal processing (Case study 10.1). Finally, interesting work has been carried out in the domain of pain assessment, which highlights some further complications in people with a neurological condition such as stroke.
Sensation
As explained in Chapter 9, attention is a major factor in the processing of information, as it helps us to direct our sensory systems towards relevant information, select appropriate information, allocate energy to process the information and regulate our attention to allow us to complete a task. Sensory information that is not attended to is poorly remembered, and, therefore, attention is a major component in the process of learning.
When we talk about sensation, what we are really referring to is the process of information coming in from the environment (internal or external) through the sense organs and being relayed to the central nervous system. The various sense organs (eyes, ears, nose, tongue, skin and proprioceptors) possess dedicated mechanisms that allow them to receive a specific form of energy from the environment (e.g. electromagnetic wavelengths of a specific range) and transduce this into nerve impulses. Transduction is the key component of sensation, as it is only after this has taken place that the nervous system can begin to process information in the form of action potentials. It is important to remember that sensory information, when it is first encountered, is in its rawest form and inherently meaningless. Assigning meaning to information requires the process of perception, which will be outlined in the next section. To be able to appreciate the complexity of sensation, we will take one example by going through the processes involved in vision. Although readers are referred to other texts (e.g. Kindlen 2003) for a description of the anatomy of the various other sense organs, and the sensory processes involved in each of these, what you should aim to remember from the section on vision are the generic principles involved in information processing.
Vision
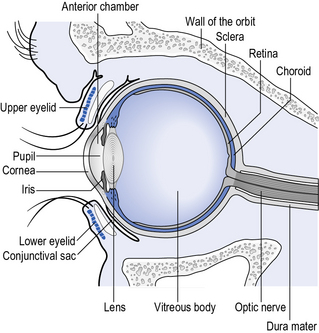
Sight is the sense through which we are able to perceive electromagnetic radiation in the form of light waves. The light waves pass into the eye through the cornea (see Fig. 10.1), which starts to curve the light waves before they pass through the lens of the eye, where further curvature results in the light being focused onto the surface of the retina.
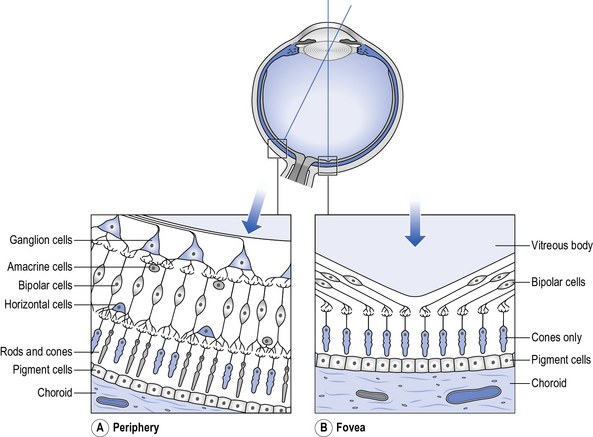
Retina
The retina (see Fig. 10.2) is a thin film of tissue lining most of the inside of the eyeball and contains blood vessels, nerve cells, photoreceptors and pigment cells. It is orangey-red in colour when viewed through an ophthalmoscope because of its blood supply and pigments. In one part of the retina a whitish patch (optic disc) can be seen, which consists of the axons of the optic nerve, i.e. the site where these axons leave the eyeball. The disc appears white because the axons here are myelinated.
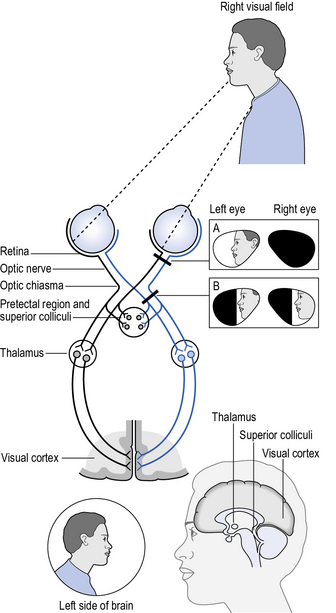
Visual pathways
The optic nerves from each eye meet up at the optic chiasma (see Fig. 10.4) where the nerve fibres carrying signals from the nasal half of the retina cross over to the other side so that information about objects on the right-hand side of the scene we are looking at (right visual field) is carried over to the left side of the brain and vice versa. If injury occurs to the visual pathway on one side of the brain after the chiasma, there will be loss of vision in one half of the visual field of both eyes, which is known as a homonymous hemianopia (see Chapter 5).