Dural Sinus Lesion, General
Bronwyn E. Hamilton, MD
Anne G. Osborn, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Arachnoid Granulations, Dural Sinuses
Dural Sinus Hypoplasia-Aplasia
Thrombosis, Dural Sinus
Dural A-V Fistula
Less Common
Meningioma
Metastasis
Lymphoma
Depressed Skull Fracture
Intracranial Hypotension
Rare but Important
Dural Venous Sinus Stenosis
Thrombophlebitis
Polycythemia
Hemangioma
Leukemia
Rosai-Dorfman Disease
Extramedullary Hematopoiesis
Lipoma
Masson Vegetant Intravascular Hemangioendothelioma
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Includes generic lesions affecting ALL dural venous sinuses
Cavernous sinus (CS) unique because of contents, proximity to skull base
Has diagnoses (e.g., perineural metastasis, aneurysm, schwannoma) that do not affect other sinuses
Imaging challenge: Differentiate dural sinus thrombosis (DST) from stenosis, anatomic variants
CTV best
MRV shows anatomical narrowing/occlusion
T2* (GRE/SWI) shows thrombus
Helpful Clues for Common Diagnoses
Arachnoid Granulations, Dural Sinuses
Can be large (> 1 cm), remodel calvarium
May narrow but not occlude sinus
Round/ovoid, well-circumscribed
CSF density/signal intensity
Dural Sinus Hypoplasia-Aplasia
Seen in up to 1/3 of normal scans
Transverse sinus (TS) most common site
“Flow gaps” on MRV can mimic DST
Confirm “flow gaps” on source data
No “blooming” thrombus on T2*
If MRV is unclear, CTV helpful
Thrombosis, Dural Sinus
Symptoms vary with extent of thrombus, collaterals, cortical vein involvement
NECT
Hyperdense clot in sinus
Cortical/subcortical hemorrhages (bilateral parasagittal if superior sagittal sinus or temporal lobe if vein of Labbe)
± Edema (vasogenic > cytotoxic)
CECT shows “empty delta sign”
MR
Loss of normal “flow void”
Clot elongated, fills sinus, shows susceptibility on T2*
Confirm with MRV
Chronic thrombosis difficult diagnosis
Progressive recanalization &/or granulation tissue forms
Chronic thrombus enhances, mimicking patent dural sinus
Dura also thickens, enhances; bizarre-appearing collaterals may mimic vascular malformation
May have clinical, imaging findings of intracranial hypertension (pseudotumor cerebri)
Dural A-V Fistula
Most acquired; clinical manifestations vary
Pulsatile tinnitus, exophthalmos
Less common = progressive encephalopathy (dementia), diffuse white matter hyperintensity from chronic venous hypertension
Imaging
Flow voids within wall of thrombosed dural sinus common
High grade lesions prone to intracranial (usually parenchymal) hemorrhage
Small web of vessels on collapsed MRA images may suggest diagnosis
DSA gold standard for diagnosis
Helpful Clues for Less Common Diagnoses
Meningioma
Enhancing dural-based mass ± “tail”
May invade, occlude, or compress dural sinuses
Bony hyperostosis variable
Metastasis
Systemic primaries may compress or invade dural sinuses
Usually arise from calvarium with secondary dural involvement
Lymphoma
Dural-based mass(es) common in metastatic lymphoma
Depressed Skull Fracture
May lacerate/compress/occlude dural sinus
± Venous epidural hematoma (EDH)
Venous EDH develops slowly, presents late!
Intracranial Hypotension
Dural venous engorgement, enhancement
Slumping midbrain, tonsillar descent, SDHs
Helpful Clues for Rare Diagnoses
Dural Venous Sinus Stenosis
Focal short segmental narrowing on CTV, MRV, or DSA (venous phase)
May cause intractable headaches (intracranial hypertension)
Patients with suspected symptomatic venous outflow restriction, pressure gradient at venography may improve after stent
Thrombophlebitis
Complication of infection (meningitis, rhinosinusitis, or mastoiditis)
Infection spreads easily due to valveless nature of intracranial venous system
May cause septic venous thrombosis
Polycythemia
High hematocrit → “dense” dural sinus
Hemangioma
Capillary/cavernous vasoformative neoplasm
Convexity dura or venous sinus (CS most common)
May present with mass effect or intracranial hypertension
Leukemia
Dural-based enhancing masses
May compress/invade dural sinuses
Rosai-Dorfman Disease
Younger patients
Lymphadenopathy > paranasal sinus disease
Lymphadenopathy usually coexists if CNS disease is present
Solitary/multiple dural-based enhancing masses
Extramedullary Hematopoiesis
Dural-based enhancing masses
Dural sinus compression/invasion rare
Lipoma
Fat in dural sinus rare; CS most common
Masson Vegetant Intravascular Hemangioendothelioma
Rare benign tumor of young patients
Papillary endothelial hyperplasia
Can cause stenosis, hypertension
Can mimic meningioma
Image Gallery
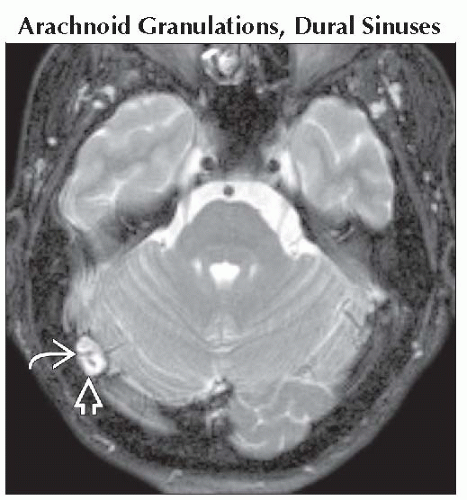 Axial T2WI FS MR shows a large ovoid CSF-signal mass  in the right transverse sinus with internal “flow void” in the right transverse sinus with internal “flow void”  , probably representing vein. , probably representing vein. |
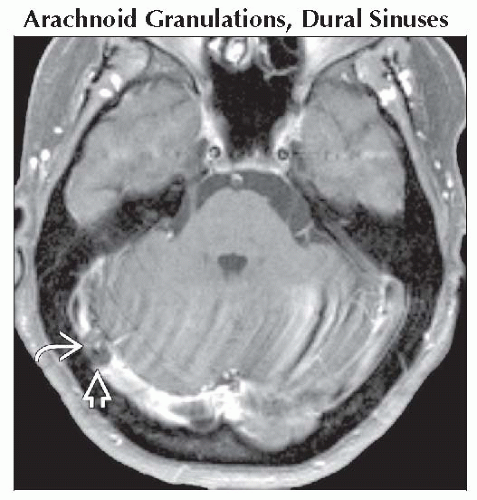 Axial T1 C+ FS MR in the same patient shows that the lesion  does not enhance and is the same signal as CSF. Vein does not enhance and is the same signal as CSF. Vein  enhances. This was an incidental finding in an asymptomatic patient. enhances. This was an incidental finding in an asymptomatic patient. |
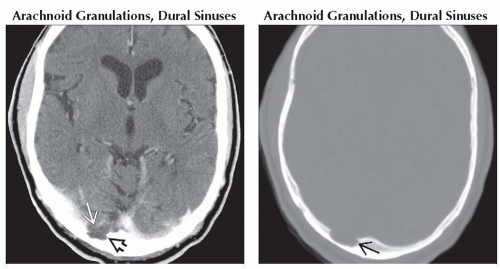 (Left) Axial CECT shows hypodense CSF-like lobulated filling defect in the right transverse sinus
 . Note adjacent calvarial scalloping . Note adjacent calvarial scalloping  . (Right) Axial bone CT in the same patient shows smooth, well-delineated erosion . (Right) Axial bone CT in the same patient shows smooth, well-delineated erosion  of the calvarium caused by arachnoid granulation. of the calvarium caused by arachnoid granulation.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|