Emerging Pharmacologic Treatments for Spinal Cord Injury
Emerging Pharmacologic Treatments for Spinal Cord Injury
Virgilio Matheus
Christopher A. Iannotti
Michael P. Steinmetz
Any insult to the spinal cord that leads to a change in its function, either temporary or permanent, is considered a spinal cord injury (SCI). The reversal of paralysis following a lesion to the spinal cord represents one of the greatest challenges for modern spine medicine. Despite significant improvements in emergency medical care, neurointensive care, and surgical management of SCI patients, as well as major advancements in our understanding of the pathophysiology of SCI, there remains a lack of effective therapies aimed at directly targeting secondary injury cascades after SCI. SCI destroys neuronal connectivity by severing descending motor and ascending sensory axonal pathways. Such damage often results in permanent paralysis and loss of sensation below the level of injury. Although SCI causes loss of neurons and glial cells at the lesion site, functional deficits result primarily from loss of white matter axons by direct trauma and from progressive damage to initially intact axons by complex secondary injury mechanisms mainly related to inflammatory processes (1). To date, numerous potential therapies have been investigated in prospective, randomized, controlled clinical trials. Despite evidence that these agents demonstrated benefit in preclinical animal studies of SCI, many of these drug therapies have been unsuccessful in demonstrating functional improvement. This chapter reviews previous clinical trials, as well as major recent preclinical advances, using pharmacologic approaches to the treatment of SCI.
SCI EPIDEMIOLOGY
SCI is associated with severe physical, psychological, social, and economic burdens on patients and their families. With an annual incidence rate of 15 to 40 persons per million, it has been estimated that at least 10,000 to 15,000 North Americans will suffer a SCI each year (2). With the average acute-care and rehabilitation charges of approximately $60,000.00 for each of these phases of care, the societal expense associated with the medical management, as well as lost earnings of this disorder over the course of one’s life is significant (3). Besides the economic burden, it is important to consider the severe psychological challenge for the patients and their families. For this and many other reasons, SCI has been considered a major public health problem. It has been estimated that the lifetime cost of medical care and other injury-related expenses for a 25-year-old patient with SCI who suffers a high cervical quadriplegia to be approximately $3 million (4). SCI predominantly occurs in young, otherwise healthy individuals, with injury occurring with the greatest frequency in those between 15 and 25 years of age; the male-to-female ratio for SCI is approximately 4 to 1 (5) Common causes of SCI in the United States are motor vehicle accidents (50%), falls and work-related injuries (30%), violent crime (11%), and sports-related injuries (9%) (6). Injuries most commonly occur in the cervical spine, and are associated with the most devastating neurologic impairments (e.g., quadriplegia). A recent report from the US National Spinal Cord Injury Database found that 56% of all SCI cases occur in the cervical spine.
PATHOPHYSIOLOGY OF SCI
A detailed understanding of the pathophysiologic processes occurring following SCI is paramount to the development of effective therapies for SCI. The pathophysiology of SCI is best described as biphasic, consisting of a primary and secondary phase of injury (7). The primary phase involves the initial, immediate mechanical injury during which failure of the spinal column occurs, and includes compression, contusion, shear, or laceration due to penetrating injury, and acute stretching of the spinal cord as a result of vertebral distraction or sudden acceleration-deceleration of the spinal column. The most common underlying primary injury mechanism results from the acute compression and contusion of the spinal cord due to bone or disk displacement within the spinal column during fracture dislocation or burst fracture of the spine (2). Multiple mechanisms of injury exist, which include damage to the spinal cord from direct trauma, compression (from bony fragments, hematoma, or disk material), and ischemia related to damage or impingement on the spinal arteries. The primary mechanical trauma to the spinal cord, along with subsequent persistent compression, triggers a complex and delayed pathologic cascade, termed the “secondary injury” phase, which involves vascular dysfunction, edema, ischemia, excitotoxicity, electrolyte shifts, free radical production, inflammation, and delayed apoptotic cell death (8). Although neurologic deficits are present immediately following the initial injury, the secondary injury phase results in a protracted period of neuroinflammation and tissue destruction. The spatial extent of secondary injury events spreads both radially and longitudinally along the spinal cord in a rostral-caudal manner, resulting in neuronal and glial cell death. The end result is cavitation of central gray matter, along with partial or complete loss of adjacent white matter tracts.
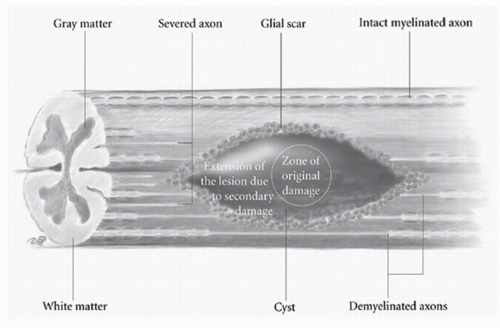
The pathophysiology of SCI has been extensively studied in many experimental animal models, including mice, rats, cats, and primates, in order to understand the cellular and molecular mechanisms of tissue damage and the consequent disability (2). Traumatic SCI initiates a series of destructive cellular inflammatory processes that accentuate tissue damage at and beyond the original site of trauma, and cystic cavitation inevitably occurs due to these secondary injury events. Contusion SCI in animals produces a predictable pattern of progressive injury resulting in neuronal and glial cell death, vascular injury, axonal destruction, and demyelination, which is analogous to the human spinal cord contusion injury, the most common type of the human SCI (Fig. 53.1) (7,9). The progressive expansion of the injury from gray to white matter causes secondary damage to initially intact axons within hours to several weeks after injury. The cellular inflammatory response, predominated by macrophages, has been implicated as the primary mediator of progressive secondary injury. The major targets for spinal cord repair include severed and/or demyelinated axons, inflammatory cells and proinflammatory cytokines, and glial scar components.
Figure 53.1. Schematic diagram depicting the various pathologic events occurring after traumatic SCI. A zone of primary injury progressively expands due to secondary injury. Acute and chronic inflammatory cascades lead to secondary tissue damage, axonal loss, and demyelination. The end result is a cystic cavity surrounded by a rim of preserved white matter. An astroglial scar forms the periphery of the lesion, presenting a physical and chemical barrier to axonal regeneration.
COMPLETED SCI CLINICAL TRIALS
To date, several therapeutic strategies have been examined in Phase I, II, and III clinical trials (Table 53.1). Ten randomized controlled trials examining methylprednisolone sodium succinate (MPSS), tirilazad mesylate, GM-1 ganglioside, thyrotropin-releasing hormone, gacyclidine, naloxone, and nimodipine have been completed and have demonstrated some promise for outcome improvement. Several clinical trials have explored various surgical interventions, such as early surgical decompression (Surgical Treatment of Acute Spinal Cord Injury Study, STASCIS) and electrical field stimulation.
EMERGING PRECLINICAL SCI THERAPIES
The failure of axonal regeneration after central nervous system (CNS) injury is the result of two distinct processes: (a) the limited intrinsic regenerative potential of CNS neurons and (b) the inhibitory extrinsic environment of the injured CNS. Experimental therapies for SCI can be grouped into several subtypes, based on their general mechanism of action. These general treatment subcategories include therapies that (a) promote neuroprotection, (b) stimulate intrinsic axonal regrowth, (c) enhance remyelination, and (d) remove/block inhibitory molecules within damaged myelin and within the astroglial scar. Multiple inhibitory molecules exist that make the injured CNS a nonpermissive environment for axonal growth. These molecules may be categorically divided into myelin-associated inhibitors and inhibitors associated with the astrocytic glial scar. Recently, major advances in molecular neuroscience have led to the identification of several growth-inhibitory molecules associated with myelin (Nogo, myelin-associated glycoprotein [MAG], oligodendrocyte myelin glycoprotein [OMgp]) and the glial scar (chondroitin sulfate proteoglycans, CSPGs), as well as their receptors and downstream signaling pathways, which comprise the inhibitory extrinsic environment of the injured CNS. This chapter will review several recently developed targeted molecular strategies that enable axons to overcome inhibitory influences of myelin-associated proteins and astroglial scar components.
TABLE 53.1 Synopsis of Previous Randomized Clinical Trials in SCI (8,10, 11, 12, 13, 14, 15, 16 and 17)
Trial
Phase
Patients
Treatment Arms
Outcome
NASCIS I USA-1984
III
330
MPSS 100 mg vs. 1,000 mg × 10 d
No difference between both arms
NASCIS II USA-1990
III
487
MPSS × 24 h, naloxone, placebo
Improvement at 6 mo if MPSS started within 8 h of injury. Naloxone negative.
Maryland GM-1 Geisler et al. USA-1997
II
34
Ganglioside (GM-1), placebo
Enhance recovery of neurologic function. Small group of patients, pilot study.
Otani et al. Japan-1994
Nonblinded trial
158
MPSS × 24 h, placebo
Similar improvement on motor function as NASCIS II but better sensory outcome.
TRH-San Francisco General Hosp. USA-1995
II
20
Thyrotropin-releasing hormone (TRH), placebo
Suggestive of improved recovery with TRH. Small group of patients, pilot study.
NASCIS III USA-1997
III
499
MPSS × 24 h MPSS × 48 h MPSS bolus + tirilazad × 48 h
Improved recovery if MPSS administered within 3 h of injury. Tirilazad not better then MPSS.
Nimodipine France-1998
III
100
Nimodipine
MPSS × 24 h
Nimodipine + MPSS 24 h
Placebo
No significant difference. Believed to be a type II error due to small sample.
Gacyclidine France-1999
II
280
Gacyclidine at low, medium and high dose vs. placebo
Negative study
Pointillart et al. France-2000
Double-blinded
106
MPSS × 24 h
Nimodipine
MPSS + Nimodipine
Placebo
No significant difference in outcome. Higher incidence of infections on MPSS treated group.
Sygen Group Study USA-2001
III
797
MPSS + placebo
MPSS × 24 h+ GM-1 low dose
MPSS × 24h + GM-1 high dose
Negative during evaluation at 26 wk. Tendency toward improvement at 52 wk.
STASCIS (pilot study) Canada-1999
III
26
Assessment of possibility for obtaining spinal CT myelo or MRI + decompression during initial 8 h following injury
Only seven patients underwent imaging and decompression during the first 12 h. Not feasibility to perform large study aiming for imaging + early decompression.
MPSS, methylprednisolone sodium succinate.
Several clinical trials have been recently initiated or planned using promising potential therapies. These therapeutic strategies, which are both pharmacologic and cell based (e.g., minocycline, C3 transferase (Rho inhibition), oligodendrocyte progenitor cell transplantation), have been validated by multiple laboratories in experimental and preclinical studies. Unfortunately, some experimental and poorly characterized SCI therapies are being offered without rigorous investigation, which will produce results of limited scientific value and risk harm to SCI patients who are understandably desperate for any intervention that might improve their function. However, recent advances have provided a basis for optimism for both patients and clinicians, as safe and effective therapies for SCI may become available over the next decade.
Considering the multifactorial nature of secondary pathologic events attributed to SCI, drug “cocktails” with multifaceted modes of neuroprotection and axonal growth promotion will likely be useful in preventing or limiting secondary injury progression. Due to the numerous complex pathophysiologic changes occurring after SCI, successful repair may involve strategies that combine the use of neuroprotective drug therapies with those that promote axonal regeneration, such as cell transplantation, genetic engineering to increase neurotrophic factors, neutralization of inhibitory factors, limiting glial scar formation, and neurorehabilitation. Furthermore, neuroprotective drug therapies that function at later time points following SCI will likely have greater clinical relevance than those with small therapeutic windows. There is also a requirement to establish methods for the systematic evaluation of preclinical therapeutic outcomes from the various research SCI centers. In the evaluation of future potential SCI therapies, a clinical basis for the implementation of novel therapies will be required. Refined clinical outcome measures, as well as neurophysiologic measures, are needed for a precise qualitative and quantitative assessment of spinal cord function in SCI patients, especially at an early stage after injury. This will allow for better detection of improvements in functional recovery and will enable clinicians to precisely monitor the effects of novel therapies (3,18).
MINOCYCLINE
Minocycline is a highly lipophilic semisynthetic derivative of tetracycline and is capable of crossing the bloodbrain barrier. Minocycline possesses anti-inflammatory properties, which are distinct from its ability to inhibit bacterial protein synthesis. Minocycline can inhibit excitotoxicity, oxidative stress, caspase-dependent and caspase-independent pathways of neuronal death, and proinflammatory mediators released by activated microglia (19). The anti-inflammatory properties of minocycline appear include reduction in the expression or activity of inflammatory cytokines, free radicals, and matrix metalloproteinases (20).
Neuroprotection by minocycline has been demonstrated in animal models of SCI. In these studies, systemically administered minocycline demonstrated convincing neuroprotective ability by decreasing apoptosis of oligodendrocytes, diminishing microglial cell activation, reducing lesion size, and improving neurologic deficit (19,20). In addition, minocycline was also shown to be a superior therapeutic agent to MPSS, and maintained neuroprotective efficacy when administered 1 hour following experimental SCI (20). Minocycline has been shown to improve functional recovery after clip compression SCI in mice and after contusion SCI in rats where it inhibits release of cytochrome c from mitochondria (19, 20, 21 and 22). After intraperitoneal (i.p.) administration of minocycline in a rat contusion model of SCI, minocycline exerts neuroprotective and antiinflammatory effects leading to a reduction in caspase-3 activation, reduced neuronal apoptosis, and improved recovery early after SCI (23). The proposed mechanisms of minocycline-mediated neuroprotection within the injured spinal cord also include increased mRNA levels of the anti-inflammatory cytokine IL-10 and decreased tumor necrosis factor-a (TNF-a) production (19). Although positive effects with minocycline have been reported in several animal models of injury with different drug administration schemes, an independent replication of the study by Lee et al. (21) using minocycline after experimental contusion SCI did not lead to significant functional or histopathologic improvements (24). Although minocycline has been demonstrated to have a good safety profile with prolonged use in humans, the use of minocycline following contusive SCI requires may require further experimental investigation before clinical trials are implemented.
Despite mixed results of minocycline in SCI animal models, a recent double-blind randomized controlled pilot study was initiated in SCI patients presenting within 12 hours after nonpenetrating injury (25). Patients were randomized to receive intravenous minocycline 200 mg bid or 400 mg bid after an 800 mg loading dose, or placebo, for 7 days. There were no adverse treatment-related effects. Minocycline treatment improved American Spinal Injury Association (ASIA) motor scores in complete and incomplete cervical SCI patients through 1 year, and improved the FIM and SF-36 scores (25). However, no differences in ASIA motor scores were observed for patients with thoracic complete SCI. Based on these results, largescale clinical trials with minocycline may be anticipated.
Only gold members can continue reading. Log In or Register to continue
 Cervical Orthoses and Cranioskeletal Traction
Cervical Orthoses and Cranioskeletal Traction



