Fig. 67.1
Empty sella syndrome. (a, b) Coronal T1-weighted gadolinium-enhanced MR images. The pituitary gland appears flattened, with increased cerebrospinal fluid (CSF) space above the gland. The optic chiasm is slightly prolapsed
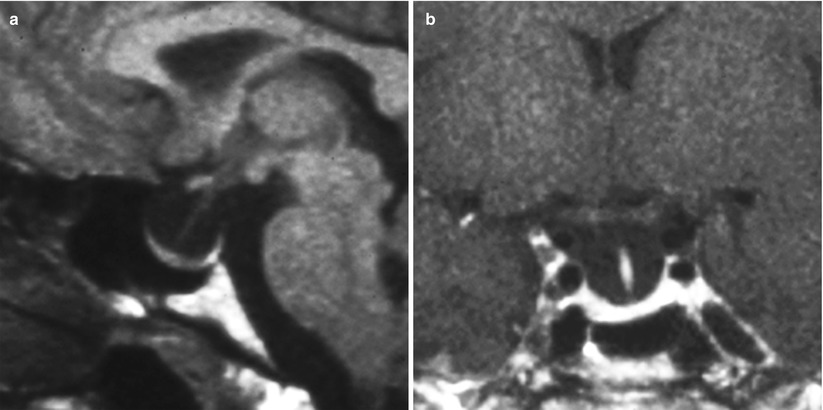
Fig. 67.2
Empty sella syndrome. (a) Sagittal T1-weighted precontrast MR image. (b) Coronal T1-weighted gadolinium-enhanced image. The pituitary gland appears flattened, with increased CSF space above the gland
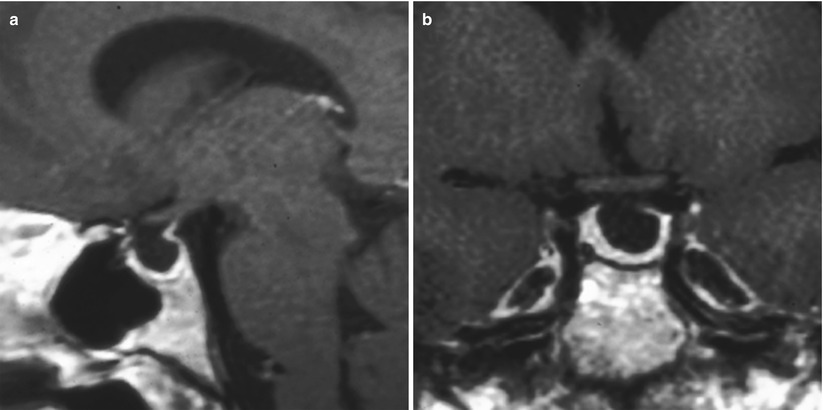
Fig. 67.3
Empty sella syndrome. (a) Sagittal T1-weighted gadolinium-enhanced MR image. (b) Coronal T1-weighted gadolinium-enhanced image. The pituitary gland appears flattened, with increased CSF space above the gland. The pituitary stalk is mildly displaced posteriorly (a)
Optic chiasm prolapse may be noted in some cases, especially in secondary empty sella syndrome following the resection of large sellar tumors.
Empty sella syndrome may be characterized as partial (65 % of patients) or complete (35 % of patients) [6].
The degree of empty sella has not been correlated to the severity of clinical symptoms [11].
67.3 Clinical and Surgical Management
The optimal management of empty sella syndrome has been controversial.
Few patients require surgical management, as an empty sella is often an incidental finding and most patients are asymptomatic at the time of diagnosis.
Conservative management is usually indicated, unless signs of intracranial hypertension, hypopituitarism, visual loss, or CSF rhinorrhea are noted.
A thorough endocrine evaluation should be performed on all symptomatic patients with empty sella syndrome.
Symptomatic patients with PES should be screened for symptoms and signs of intracranial hypertension (papilledema, headache, visual symptoms). Medical management may be indicated, including weight loss and possible carbonic anhydrase inhibitors.
Patients with suspected or documented intracranial hypertension and those with CSF rhinorrhea may require insertion of a CSF-diverting shunt, transsphenoidal repair of a sellar floor defect, or both.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








