31 Endoscopic Transethmoid-Pterygoid-Sphenoid Approach
Davide Locatelli, Ilaria Acchiardi, Matteo Vitali, Frank Rikki Canevari, and Paolo Castelnuovo
 Introduction
Introduction
The transethmoid-pterygoid-sphenoid (TPS) approach provides surgical access to lateral regions of the anterior and middle cranial base and to the infratemporal fossa. It is an extended application of the endoscopic transethmoid approach.
 Indications and Advantages
Indications and Advantages
A TPS approach is indicated for all pathologies with lateral extension to the course of the internal carotid artery at the base of the skull, such as cerebrospinal fluid (CSF) fistulas of Sternberg’s canal,1,2 pituitary macroadenomas, cranial pharyngiomas, chordomas and chondrosarcomas, meningiomas, tumors of the sellar cavity (metastases), angiofibromas, and retrobulbar, dermoid, and epidermoid tumors.3
 Contraindications
Contraindications
There are no absolute contraindications to using a TPS approach, although, in view of the importance of anatomical landmarks in the various stages of surgery, any alteration in normal anatomy is a risk factor, such as the recurrence of lesions after previous surgical procedures.
Another risk factor is alteration in vessel walls. For this reason, patients who have undergone previous radiotherapy or patients with lesions involving the tunica adventitia of vessels should be carefully assessed prior to surgery.
 Surgical Planning
Surgical Planning
Surgical planning entails gadolinium-enhanced magnetic resonance imaging (MRI) of the lesion, maxillofacial computed tomography (CT), and three-dimensional (3D) CT angiography. If necessary, a carotid occlusion test is done (Figs. 31.1, 31.2, 31.3, and 31.4).
 Surgical Approach
Surgical Approach
The transethmoid-pterygoid-sphenoid approach involves four main surgical steps:
1. The ethmoid step
2. The pterygoid step
3. The pterygoid-sphenoid step
4. The intracavernous step
The Ethmoid Step
This step involves anterior-posterior ethmoidectomy, sphenoidectomy, and partial removal of the middle and superior turbinates. The anatomical structures and the surgical phases are well known and are the same as those involved in sinonasal phlogistic diseases, albeit with some specific technical details. First, the anterior ethmoid region is explored, and the inferior tip of the uncinate is identified and removed with a backward-cutting punch, using the inferior middle margin of the ethmoid bulla as a landmark. Once partial inferior uncinectomy has been performed and the infundibulum opened, the natural ostium of the maxillary sinus can be explored. The uncinate process can be completely removed with angled forceps and a microdebrider. The inferior medial margin of the bulla is exposed, opened, and removed in a mediolateral direction as far as the lamina papyracea. Once the bulla has been removed, the natural ostium of the maxillary sinus is widened posteriorly. Following anterior ethmoidectomy, the second portion of the middle turbinate is opened from the inferomedial margin to the lamina papyracea, providing access to the posterior ethmoid. The next step consists of partially resecting the middle turbinate with cutting forceps starting from the sagittal portion. The superior insertion of the middle turbinate and the lateral edges, with the branches of the sphenopalatine artery, are preserved.
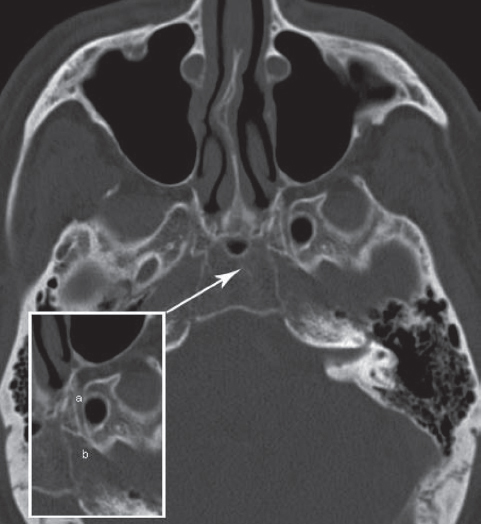
Fig. 31.1 Axial computed tomography (CT) of the skull base showing the vidian canal (a) and the internal carotid artery (b).
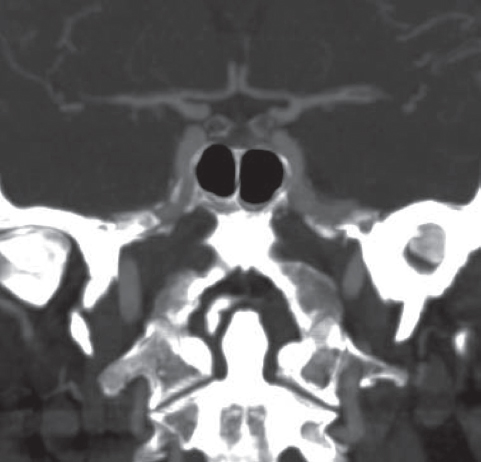
Fig. 31.2 Angio-CT with visualization of the paraclival carotid artery bilaterally.
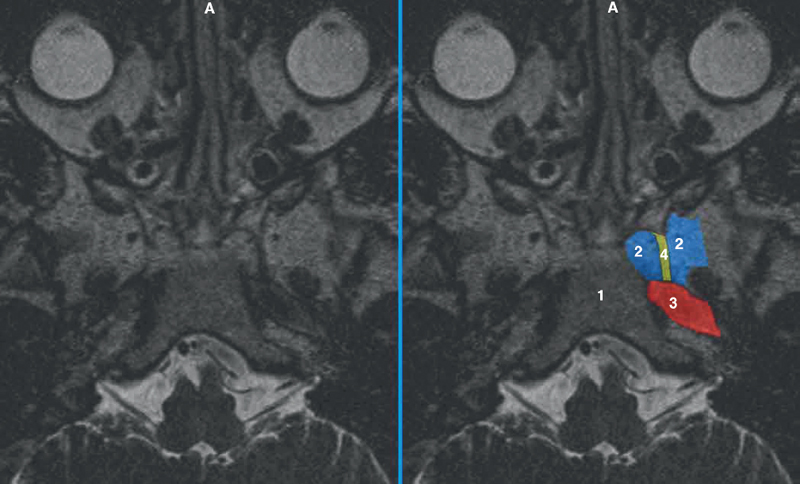
Fig. 31.3 Axial T2-weighted magnetic resonance imaging (MRI) sequence at the level of the vidian canal: 1, clivus; 2, pterygoid; 3, horizontal tract of the internal carotid artery (ICA); 4, vidian canal.

Fig. 31.4 Multiplanar reconstruction (MPR) of the T2-weighted MRI sequence showing the vidian canal and the internal carotid artery.
The sagittal portion of the superior turbinate is identified and removed in an anterior-to-posterior direction up to its posterior insertion into the anterior sphenoid wall, preserving the superior portion of the basal lamella. The natural ostium of the sphenoid sinus opens medial to the tip of the superior or supreme turbinate and is then widened using a circular cutting punch. Once the sphenoid has been explored, the sphenoidectomy is extended laterally until the orbital apex is identified (Fig. 31.5). Technical expertise in this stage lies in identifying the lamina papyracea and orbital apex, which defines the upper boundary of the TPS approach.4–6
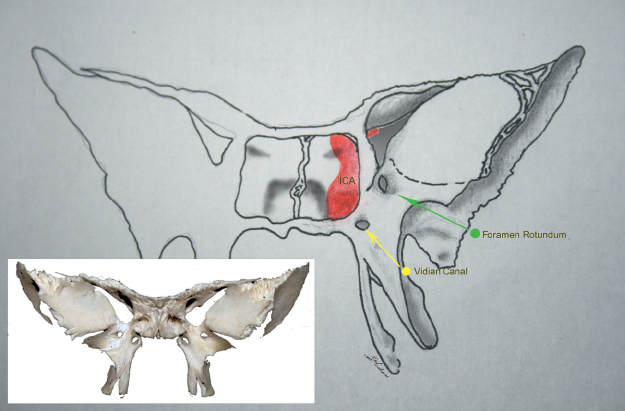
Fig. 31.5 Schematic drawing of the sphenoid bone and of the landmarks correlated with the picture of the sphenoid (inset).
Related posts:
 Anesthesia in Endoscopic Skull Base and Brain Surgery
The Endonasal Transplanum-Transtuberculum Endoscopic Approach in Pituitary Adenomas
Endoscopic Transnasal Craniectomy and the Resection of Extensive Craniopharyngiomas
External Versus Endoscopic Approaches for Skull Base Malignancies
Combined Cranio-Endoscopic Approach
Anatomy of the Orbit and Related Structures
Anesthesia in Endoscopic Skull Base and Brain Surgery
The Endonasal Transplanum-Transtuberculum Endoscopic Approach in Pituitary Adenomas
Endoscopic Transnasal Craniectomy and the Resection of Extensive Craniopharyngiomas
External Versus Endoscopic Approaches for Skull Base Malignancies
Combined Cranio-Endoscopic Approach
Anatomy of the Orbit and Related Structures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


