Enlarged Vertebral Body/Posterior Element
Lubdha M. Shah, MD
DIFFERENTIAL DIAGNOSIS
Common
Facet Arthropathy
Facet Arthropathy, Cervical
Facet Arthropathy, Lumbar
Baastrup Sign
Paget Disease
Aggressive Hemangioma
Compensatory Enlargement
Scoliosis
Spondylolysis
Congenital Fusion
Less Common
Metastases, Lytic Osseous
Aneurysmal Bone Cyst
Osteoblastoma
Chordoma
Rare but Important
Fibrous Dysplasia
Chondrosarcoma
Osteochondroma
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Osteoblastoma should always be considered in the differential diagnosis of painful scoliosis
Center of the lesion in the vertebral body vs. posterior element may help with the differential diagnosis
Helpful Clues for Common Diagnoses
Facet Arthropathy, Cervical
Capsular laxity and joint space narrowing may lead to degenerative spondylolisthesis
Osteoarthritis of synovial-lined zygapophyseal joints
Hypertrophic changes with osteophytes, normal bone mineralization, & joint space narrowing
Facet Arthropathy, Lumbar
Osseous hypertrophy with articular joint space narrowing and encroachment upon neural foramen
Irritation of synovium produces synovial hyperplasia with paradoxical joint space widening
Facet arthrosis syndrome with low back, hip, and buttock pain aggravated by rest
Baastrup Sign
Close approx. & contact of adjacent spinous process with reactive sclerosis, enlargement & flattening of apposing interspinous surfaces
“Kissing” spinous processes
Cystic degeneration of interspinous ligaments and posterocentral epidural cyst
Paget Disease
Enlarged vertebra and neural arch with diffusely coarsened & haphazard bony trabecular pattern
Most commonly L3 & L4
Cortex is thickened
Anterior concavity of the vertebral body is lost
Can cause spinal stenosis & neural foraminal narrowing
No epidural soft tissue component unless sarcomatous degeneration
Aggressive Hemangioma
Expanded & indistinct cortex, irregular honeycombing pattern, & soft tissue mass
Trabecular condensation thinner in comparison to Paget disease
Lesions commonly involve entire vertebral body with extension into neural arch
Typically occur between T3 & T9
Epidural extension may cause cord compression
Can become symptomatic with growth, which often occurs during pregnancy
Compensatory Enlargement
Scoliosis
Minimal structural vertebral deformities & advanced degenerative changes
Facet osseous overgrowth, asymmetric disc space, & discogenic sclerosis at the concave aspect of the scoliosis
Unilateral radicular symptoms on the side of the concavity of the deformity
Spondylolysis
Defects in pars interarticularis (PI) may be due to repetitive stress injury
Spinal canal is elongated at the level of the pars defect on axial imaging
Most common at L5
Sclerosis of PI, volume averaging of superior facet spur, partial facetectomy, blastic metastases may mimic spondylolysis
Congenital Fusion
Vertebral bodies smaller than normal with tapered contour at fused disc space
Rudimentary disc space with reduced height & diameter, “wasp waist”
Degenerative changes at adjacent levels
± Fusion of posterior elements
Helpful Clues for Less Common Diagnoses
Metastases, Lytic Osseous
50-70% bone destruction required for detection on radiography
Lesion involves posterior cortex & pedicle
Diffuse involvement of marrow gives the appearance of brighter disc than bone on T1WI
Fat suppression on enhanced T1WI helpful to unmask lesions
Aneurysmal Bone Cyst
Arise in the neural arch with the majority (75-90%) extending into the vertebral body
Expansile remodeling of bone with cortical thinning
Fluid-fluid levels with hemorrhage
No tumor matrix
Osteoblastoma
Originate in the neural arch, often extend into the vertebral body
> 1.5 cm (osteoid osteoma < 1.5 cm)
Narrow zone of transition with sclerotic rim
Bone matrix on CT or radiograph
May be associated with an aneurysmal bone cyst (10-15%)
Painful scoliosis (50-60%)
Chordoma
Rare involvement of the vertebral body
Purely lytic
T2 hyperintense with multiple septations
Variable enhancement
Amorphous intratumoral Ca++ in 30% of vertebral lesions
Helpful Clues for Rare Diagnoses
Fibrous Dysplasia
Neural arch involvement > vertebral body
Spine involvement in polyostotic disease
Mildly expansile lesion with characteristic ground-glass matrix
Heterogeneous T1 & T2 signal and enhancement
Chondrosarcoma
Lytic, destructive lesion with cortical destruction and extension into the soft tissues
± Chondroid matrix (50%) of “rings & arcs”
Osteochondroma
Sessile or pedunculated osseous lesion contiguous with the parent vertebra
Cartilaginous cap > 1.5 cm in adults concerning for malignant transformation
Image Gallery
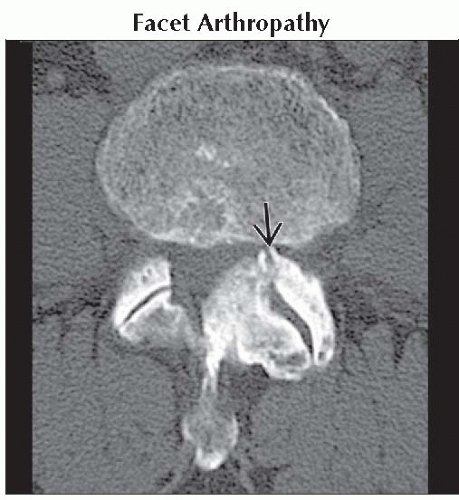 Axial bone CT shows severe left unilateral facet overgrowth
 , causing moderately severe central stenosis. , causing moderately severe central stenosis.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
