31 Evoked potentials
Sensory Evoked Potentials
Visual evoked potentials
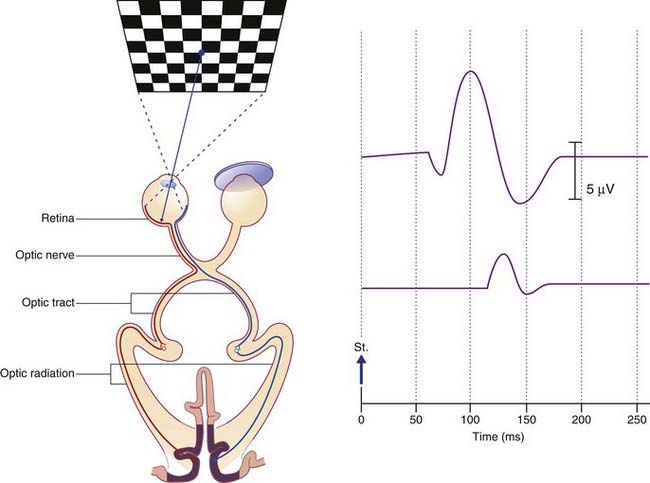
The wave peak of interest is called P100. In healthy subjects it is a positive deflection 100 ms poststimulus (Figure 31.1). In the clinical example shown, taken from a patient with a presumptive diagnosis of multiple sclerosis, the normal P100 wave from the right-eye test indicated that both optic tracts and both optic radiations were clear. The P100 wave from the left eye was both delayed and of reduced amplitude, suggesting presence of one or more plaques of myelin degeneration in the left optic nerve. (Note: On screen and in printouts, it is now customary for the waveforms to be ‘flipped’, with positive responses registering as upward deflections.)
Brainstem auditory evoked potentials
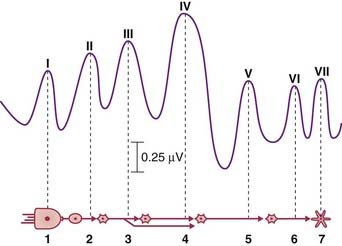
A sequence of seven averaged-out waves (I–VII) constitutes the BAER (brainstem auditory evoked response). They are accounted for in the caption to Figure 31.2.