To those I address, it is unnecessary to go farther, than to indicate that the nerves treated of in these papers are the instruments of expression, from the smile upon the infant’s cheek to the last agony of life.
I. V CRANIAL NERVE MOTOR FUNCTION: CHEWING
A. Functional anatomy of chewing
1. Motor-wise, cranial nerve (CrN) V only chews. Its motor axons innervate all and, for clinical purposes, only the chewing muscles: masseter, temporal, and lateral and medial pterygoids. CrN V conveys no efferents to glands or smooth muscle and no special sensory afferents (Table 2-7).
2. Jaw closure
a. Place your fingertips about 2 cm above and in front of the angle of your mandible. Bite hard and relax several times. The muscle felt, the masseter, is the easiest of the chewing muscle to palpate.
b. The other jaw-closing muscles are the temporalis muscles that originate in the temporal fossa and insert on the mandible and the medial pterygoid muscle.
3. Lateral jaw movement: Move your jaw from side to side. Chewing requires not only jaw closure but also a lateral, grinding action and jaw opening, caused by the lateral pterygoid muscles.
a. In Fig. 6-1 notice that the lateral pterygoid muscle originates from the skull base and inserts near the mandibular condyle.
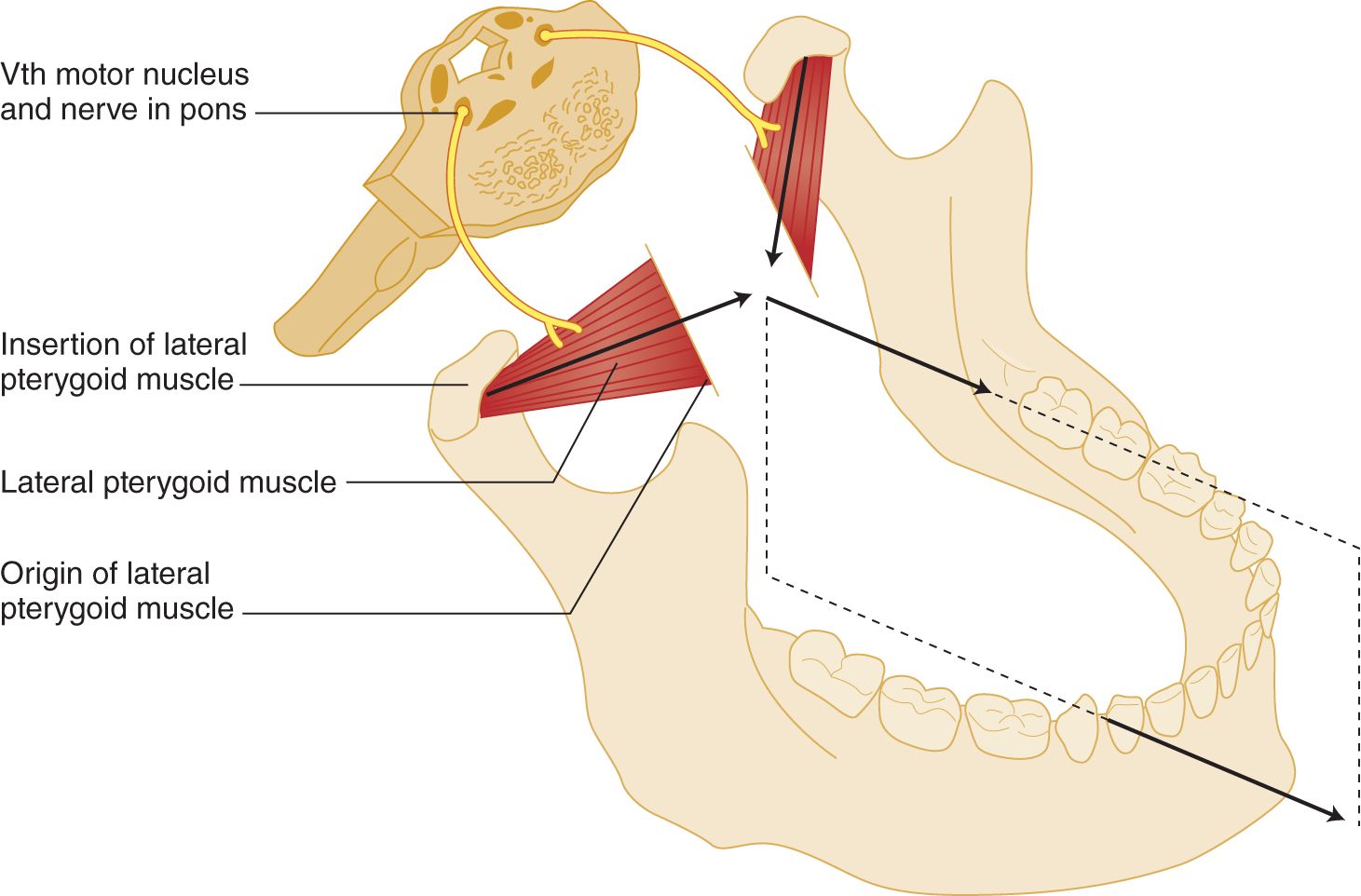
FIGURE 6-1. Innervation and action of the lateral pterygoid muscles. If both muscles contract equally, the tip of the mandible moves straight forward. If one muscle contracts, the tip moves forward and to the opposite side. Study the vector diagram (arrows between the muscles).
b. Because the skull base is fixed, only the mandible moves when the pterygoids contract. Equal contractions of right and left pterygoids pull the mandible straightforward (Fig. 6-1).
c. If only the right lateral pterygoid muscle contracts, the mandibular tip moves to the  right/
right/ left. (
left. ( left)
left)
d. If the patient (Pt) can move the jaw to the right but not to the left, the lateral pterygoid muscle on the  right/
right/ left is paralyzed. (
left is paralyzed. ( right)
right)
e. As a second action, the lateral pterygoid muscles act to open the jaw because they insert on the neck of the mandible (Fig. 6-2).
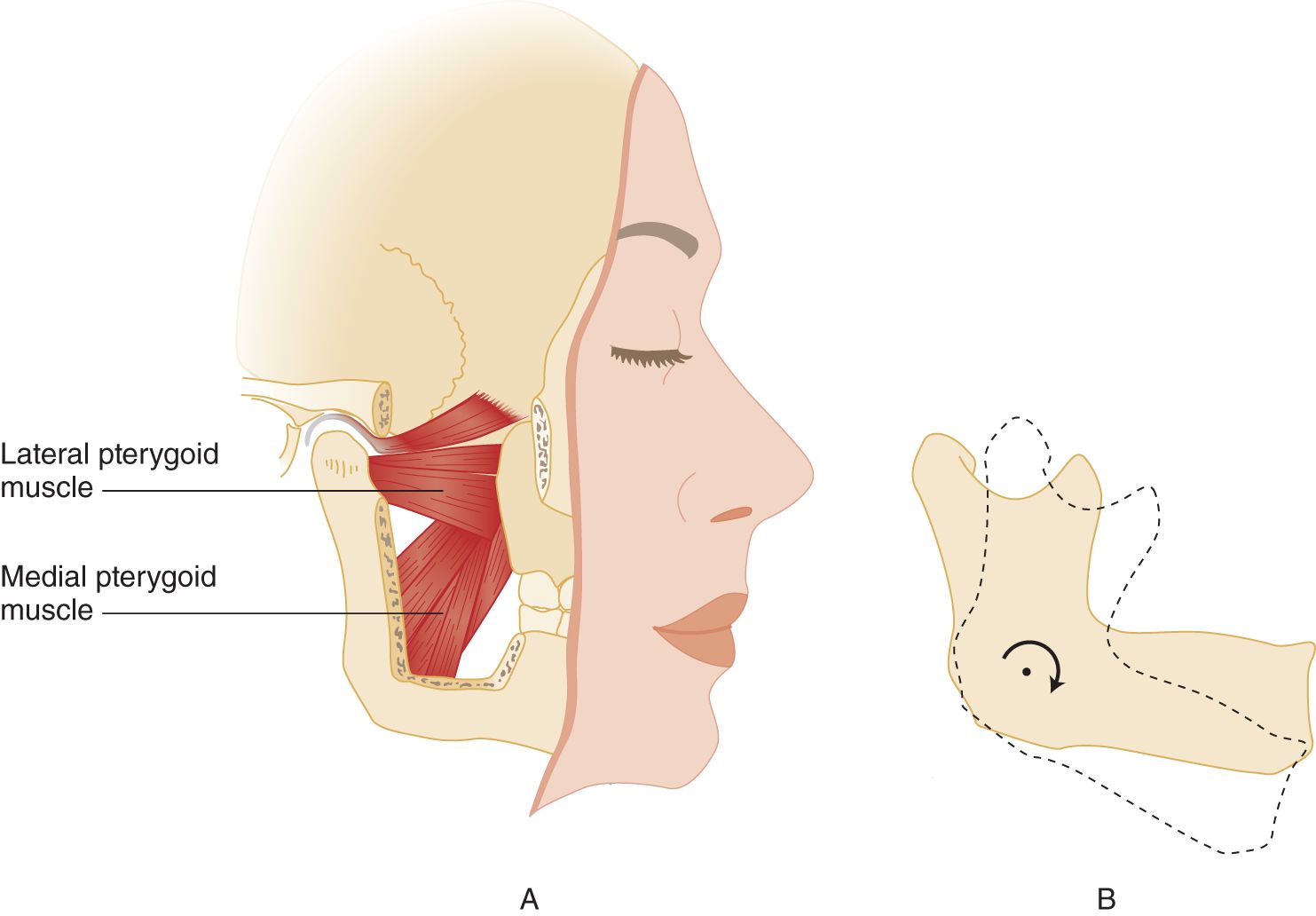
FIGURE 6-2. (A) Action of lateral pterygoid muscles to depress the tip of the mandible when the patient forcefully opens the jaw. The forward pull of the lateral pterygoid muscles also opens the jaw because the jaw is suspended to rotate around a lateral axis. (B) Arrow indicates the rotation.
f. If the Pt’s mandible moves forward and down in the midline on jaw opening, both _________
g. If the left lateral pterygoid muscle contracts, the tip of the mandible moves not only to the  right/
right/ left but also
left but also  up/
up/ down. (
down. ( right;
right;  down)
down)
4. Name the two major actions of the lateral pterygoid muscles.
_________
5. The remaining mandibular muscles innervated by CrN V all close the jaw. Name these muscles.
_________
B. Lower motoneuron lesions of cranial nerve V
1. Unilateral destruction of the perikarya or axons of CrN V causes complete paralysis of all ipsilateral chewing muscles.
2. The denervated muscle undergoes atrophy. Atrophy and paralysis are the two outstanding signs of lower motoneuron (LMN) lesions (Video 6-1). Which chewing muscle can you most readily palpate to check for atrophy? _________

Video 6-1. Atrophy of masticatory muscles in a patient with a remote history of nasopharyngeal carcinoma treated with chemotherapy and radiation.
C. Upper motor neuron innervation of cranial nerve V
1. Pursuant to general principles, one cerebral hemisphere sends upper motoneuron (UMN) axons to the contralateral V nerve nucleus. However, the contralateral innervation law requires some qualification. Compare your inability to contract half of your anal sphincter or half of your throat with the ease with which you flex a finger. These proximal (axial) muscles, such as those for trunk extension, chewing, and swallowing, that customarily act symmetrically much of or all the time usually receive about the same number of crossed and uncrossed UMN axons. The law of contralateral innervation holds best for independent unilateral movements, such as those of the hand. Hence, we find that:
a. Many proximal (axial) muscles that ordinarily contract symmetrically have  mostly ipsilateral/
mostly ipsilateral/ bilateral/
bilateral/ mostly contralateral UMN innervation. (
mostly contralateral UMN innervation. ( bilateral)
bilateral)
b. The distal (appendicular) muscles that ordinarily contract unilaterally have mainly  ipsilateral/
ipsilateral/ bilateral/
bilateral/ contralateral UMN innervation. (
contralateral UMN innervation. ( contralateral)
contralateral)
2. Because of bilateral UMN innervation, unilateral UMN lesions do not cause a severe or enduring unilateral paralysis of the chewing muscles (Willoughby and Anderson, l984). UMN lesions, as a rule, do not selectively paralyze individual muscles or sets of muscles innervated by one peripheral nerve.
D. Clinical tests of cranial nerve V motor function
1. Inspection: Inspect the temples and cheeks for atrophy of the temporalis and masseter muscles. The temporal muscle fills out the temple. Even when the Pt bites, the muscle is difficult to palpate, but after temporalis muscle atrophy, the temple sinks in. In myotonic dystrophy, the chewing muscles and sternocleidomastoid muscles atrophy. Review Fig. 1-13I. The masseters of some individuals undergo hypertrophy and stand out strongly.
2. Palpation: To test for masseter atrophy, ask the Pt to clench the teeth together strongly and unclench several times, while you simultaneously palpate the muscles of the two sides as they mound up and relax under your fingertips.
3. Testing for weakness of jaw closure.
a. Ask the Pt to clench the teeth strongly.
b. Place the heel of one palm on the tip of the Pt’s mandible and the other hand on the Pt’s forehead. Press hard on the tip of the mandible. You must brace the Pt’s head with your opposite hand because jaw closure is a very strong movement and you do not want to test the strength of the neck muscles and jaw closure at the same time. The principle is to test the strength of one muscle or one limited set of muscles at one time.
c. If the Pt complains of fatigability when chewing, as in myasthenia gravis, have the Pt chew for a period before testing.
4. Testing for weakness of the lateral pterygoid muscles.
a. Ask the Pt to forcefully open the jaw. Note whether its tip aligns with the crevice between the upper, medial incisor teeth. Weakness of one lateral pterygoid muscle would cause the jaw to deviate to the  ipsilateral/
ipsilateral/ contralateral side. (
contralateral side. ( ipsilateral (Fig. 6-2))
ipsilateral (Fig. 6-2))
b. Then ask the Pt to move the jaw from side to side.
c. Ask the Pt to hold the jaw forcefully to the side as you try to push it back to the center with the heel of your palm. Brace the Pt’s head by pressing your other hand against the opposite cheekbone.
5. A word of caution: Do not jerk or apply sudden force in testing jaw muscles, particularly in elderly or edentulous Pts. The temporomandibular joint may dislocate.
6. To ensure that you can do it, test V nerve motor function on yourself and on a partner. Do not just sit there: get up and do it! The text cannot substitute for the proprioceptive experience provided by using your own hands.
E. Analyze this 46-year-old man’s difficulty in chewing
Examination disclosed atrophy and paralysis of the left temporal and masseter muscles. When he opened his jaw, it deviated to the left. He could not move it forcefully to the right. No other muscles were weak. The evidence points to  an LMN/
an LMN/ a UMN lesion on the
a UMN lesion on the  right/
right/ left/
left/ both sides. Explain. (
both sides. Explain. ( an LMN;
an LMN;  left.)
left.)
_________
_________
_________
The paralysis affects the muscles of one nerve, CrN V. The paralysis is complete, and the muscles are atrophic. Because the atrophic and paralyzed muscles are on the left, the lesion interrupts the left V nerve.
II. VII CRANIAL NERVE MOTOR FUNCTIONS
A. Functional anatomy of facial movements
1. Except for the mandible and eyelid elevation, CrN VII innervates every other movement that the face can make. (For now study only the LMNs of VII nerve in Fig. 6-3.)
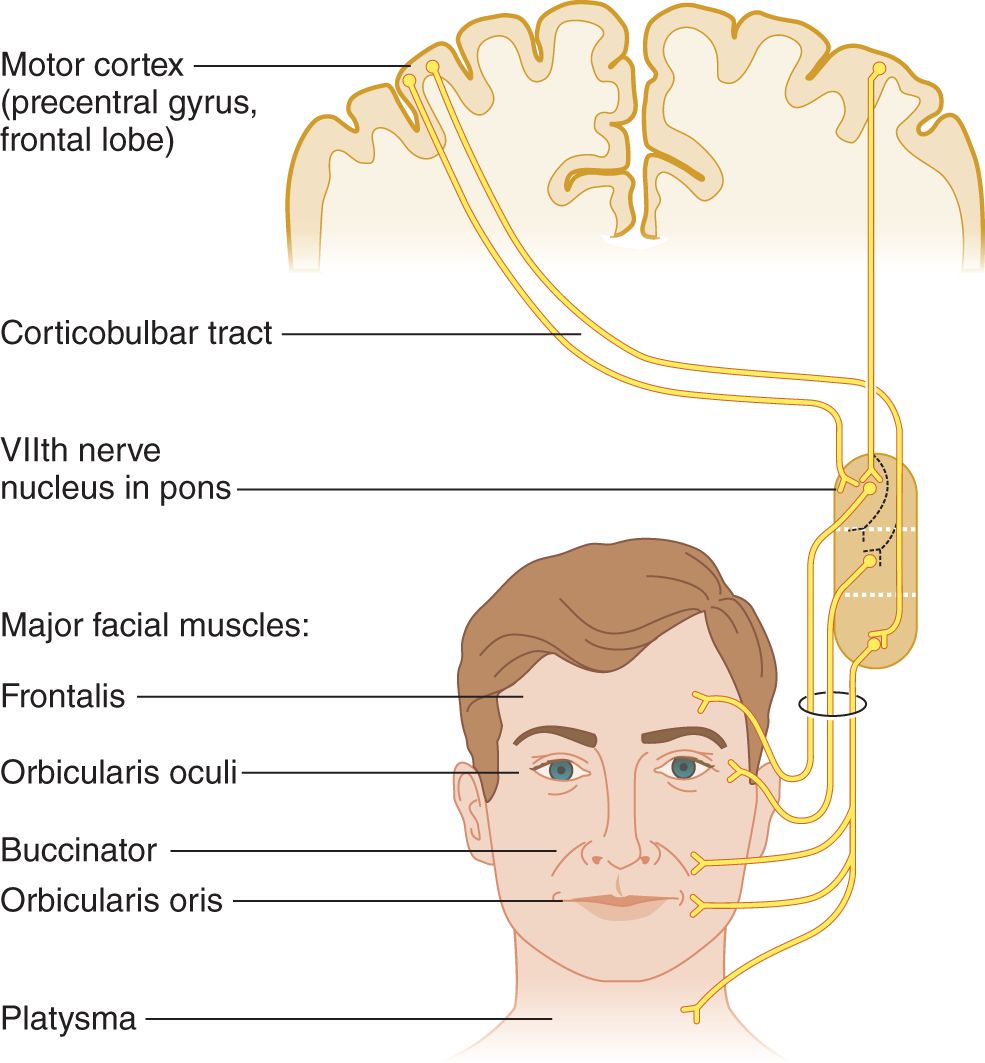
FIGURE 6-3. Upper and lower motoneuron innervations of the facial muscles. The dotted lines indicate that the number of crossed and uncrossed axons to the orbicularis oculi muscles vary from person to person. Therefore, the degree of weakness of the muscle differs after upper motoneuron lesions.
2. Look into a mirror and make every possible facial movement, including wiggling your nose and ears. (Which CrN do you suppose your dog uses to perk up his ears?)
3. Work through Table 6-1. Look into the mirror as you follow the commands the examiner (Ex) uses to test the facial muscles.
TABLE 6-1 • Summary of Tests of the Facial Muscles Innervated by Cranial Nerve VII
Examiner’s command | Observation | Muscle tested |
“Wrinkle up your forehead” or “Look up at the ceiling” | Inspect for asymmetry | Frontalis |
“Close your eyes tight and do not let me open them” | Inspect for asymmetry of wrinkles; try to pull eyelids apart | Orbicularis oculi |
“Pull back the corners of your mouth, as in smiling” | Inspect for asymmetry of nasolabial fold | Buccinator |
“Wrinkle up the skin on your neck” or “Pull down hard on the corners of your mouth” | Inspect for asymmetry | Platysma |
4. Functions of the facial muscles
a. Expression of emotions, such as when frowning and smiling.
b. Compression of lips for whistling, blowing, and spitting; labial sounds of speech; swallowing and other feeding actions.
c. Controlling and protecting the facial apertures: the palpebral fissures, oral fissure, nares, lips, and external auditory canals.
d. Dampening excessive movement of the ossicles by stapedius muscle contraction during loud sounds. After stapedius paralysis, ordinary sounds may seem uncomfortably loud, a symptom called hyperacusis.
B. Intra- and extra-axial anatomy of cranial nerve VII
1. Learn Fig. 6-4 and compare it with the generalized brainstem section in Fig. 2-14.

FIGURE 6-4. Transverse section at the caudal level of the pons that includes cranial nerve VI and VII nuclei.
2. Notice the peculiar internal loop of CrN VII around the VI nerve nucleus. Use a colored pencil to draw in the course of CrNs VI and VII on the opposite side of Fig. 6-4.
3. The pontine tegmentum contains motor nuclei for three CrNs: ____, ____, and ____. (V; VI; VII (Fig. 2-21))
4. Through the basis of the pons run the _________
5. Before exiting from the pons, the VII nerve fibers loop around the nucleus of the ____th CrN. (VI)
6. Three CrNs exit at the pontomedullary sulcus. In ventrodorsal order, these nerves are ____, ____, and ____. (VI; VII; VIII (review Fig. 2-20 if you erred))
7. As typifies peripheral nerves, the VII nerves do not cross the midline.
8. If a lesion destroys the VII nerve nucleus, the intra-axial course of the axons, or the peripheral nerve trunk, the result is paralysis of all facial muscles  ipsilaterally/
ipsilaterally/ contralaterally. (ipsilaterally)
contralaterally. (ipsilaterally)
9. The only sensory function of CrN VII tested clinically is taste (Chapter 8).
10. Mnemonics for remembering CrN VII functions: At first glance, mastery of CrN VII seems hopeless. See Fig. 6-5.
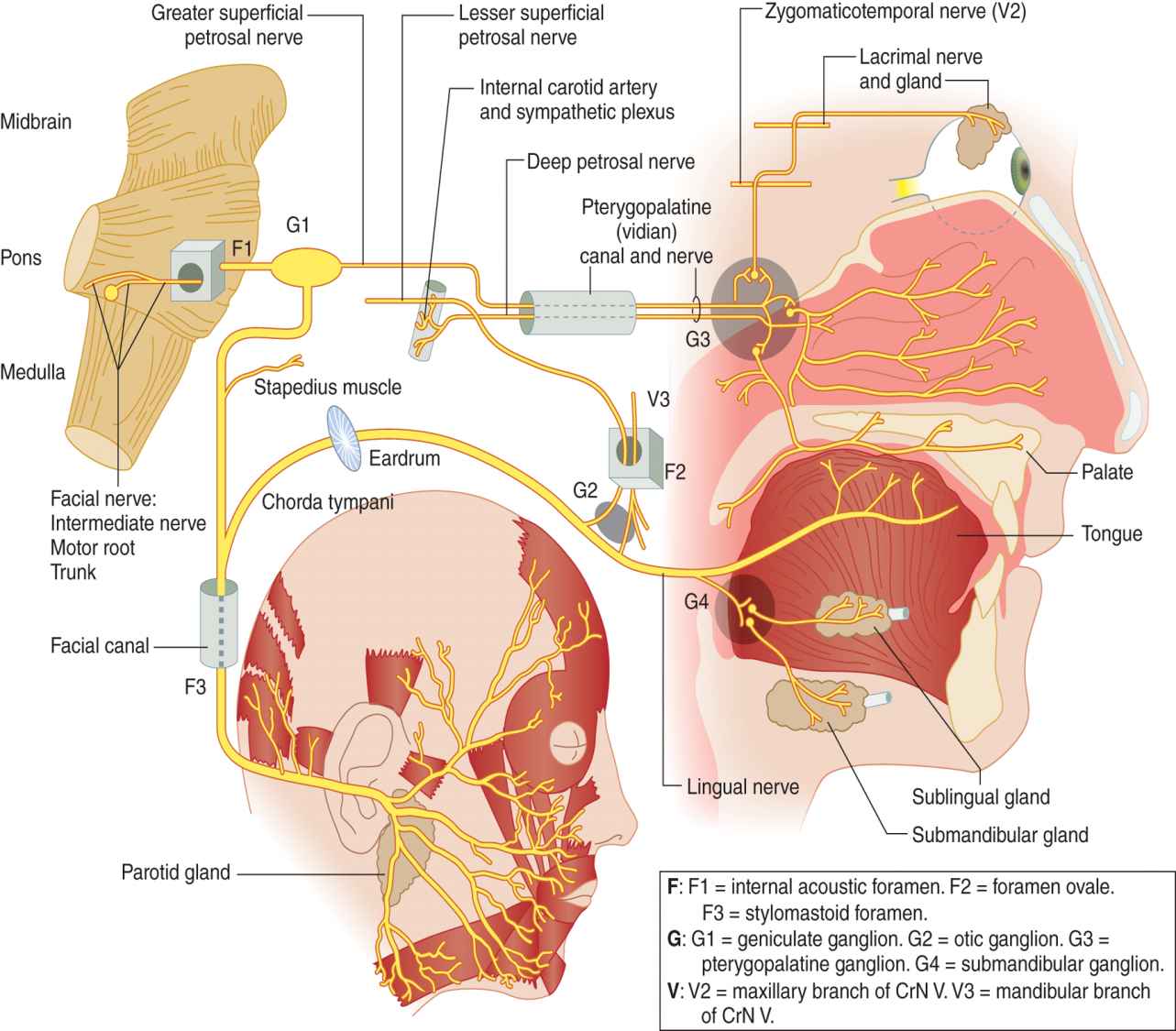
FIGURE 6-5. Diagram of the complete distribution of cranial nerve VII. (Reproduced with permission from DeMyer W. Neuroanatomy. 2nd ed. Baltimore MD: Williams & Wilkins, 1998.)
a. Salvation comes from considering CrN VII as three nerves, a branchiomotor nerve (Fig. 6-6A), a secretomotor nerve (Fig. 6-6B), and a taste nerve (Fig. 6-6C).
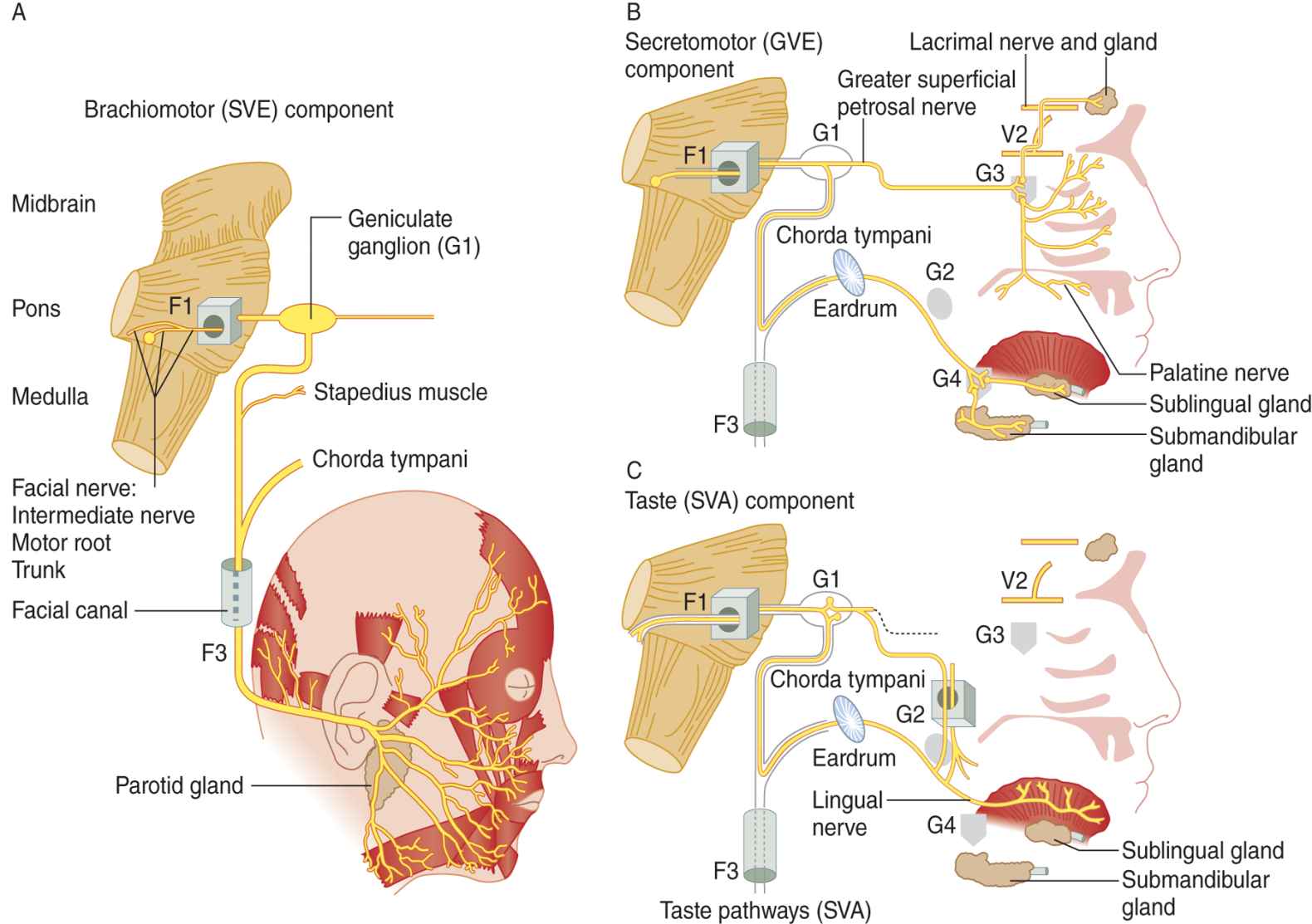
FIGURE 6-6. Diagram of cranial nerve VII as composed of three nerves: (A) a branchiomotor nerve, (B) a secretomotor nerve, and (C) a taste nerve. (Reproduced with permission from DeMyer W. Neuroanatomy. 2nd ed. Baltimore, MD: Williams & Wilkins, 1998.)
b. Remember that, in addition to moving the face, CrN VII innervates:
i. Tasting: taste from the anterior two-thirds of the tongue via the geniculate ganglion.
ii. Snotting: parasympathetic axons to the nasal mucosa via the pterygopalatine ganglion.
iii. Tearing: parasympathetic axons to the lacrimal gland via the pterygopalatine ganglion.
iv. Salivating: parasympathetic axons via the submandibular ganglion.
c. Complete interruption of CrN VII proximally causes ipsilateral facial paralysis, xerophthalmia, loss of nasal secretions, loss of taste, xerostomia, and hyperacusis.
d. Lesions can affect various sites distally along the course of CrN VII, causing the clinical signs to differ. The Ex can reason out the lesion site by “thinking along” the course of the VIIth nerve. For example, interruption of CrN VII at the facial canal (see facial canal in Fig. 6-5) would cause ipsilateral facial paralysis, but not the other clinical signs of a proximal lesion. An acute monosymptomatic LMN paralysis of the facial muscles, independent of etiology is called Bell palsy in many Anglo American countries (Peitersen, 2002) (Videos 6-2 and 6-3).

Video 6-2. Recurrent peripheral facial paralysis in a patient with a sixth nerve (CN VI).

Video 6-3. Bilateral sequential Bell’s palsies in a patient with aberrant regeneration and excessive involuntary facial movements.
e. In the Guillain–Barré syndrome (GBS), a bilateral LMN facial palsy may occur (facial diplegia). Sarcoidosis and Lyme disease also may cause bifacial palsy of the LMN type (May and Schaitkin, 1999).
C. Upper motoneuron innervation of cranial nerve VII and upper motoneuron paralysis of the face
1. By knowing the degree of unilaterality of various facial movements, you can unravel the pattern of UMN paralysis and fix it in your memory forever (Fig. 6-3).
2. As you watch in your mirror, make the movements listed in Table 6-2.
TABLE 6-2 • Tests for Unilaterality of Facial Movements
Movement | Result |
Retract one corner of your mouth at a time. | Every normal person can do it; the movement is unilateral. |
Wink one eye at a time; watch in your mirror for simultaneous contraction of the opposite orbicularis oculi muscle. | Most can do it, but some cannot wink one eye without the other; when one eye winks, the opposite orbicularis oculi contracts to some degree. |
Elevate one eyebrow at a time. | Few can do it unilaterally, but everyone can elevate them together; the movement is essentially bilateral. |
a. The freest unilateral facial movement normally is  forehead elevation/
forehead elevation/ eyelid closure/
eyelid closure/ lip retraction. (
lip retraction. ( lip retraction)
lip retraction)
b. The least free unilateral facial movement normally is  forehead elevation/
forehead elevation/ eyelid closure/
eyelid closure/ lip retraction. (
lip retraction. ( forehead elevation)
forehead elevation)
c. The utility of the various facial movements explains the gradient of unilaterality. Notice when eating that you make unilateral movements to manipulate food and clear it from your cheeks (buccinator muscle). Indeed a major discomfort of a facial palsy is that food lodges in the cheek. Unilateral forehead movements offer no such utility, and we usually activate both sides of the forehead equally. Although the eyes usually blink together, sometimes you do need to close only one. Thus, the utility of unilateral eyelid action falls between that of mouth retraction and forehead wrinkling.
3. Body parts such as the hand and lip that have the freest, most independent unilateral movements receive their UMN innervation  equally from each hemisphere/
equally from each hemisphere/ mainly from the contralateral hemisphere/
mainly from the contralateral hemisphere/ mainly from the ipsilateral hemisphere. (
mainly from the ipsilateral hemisphere. ( mainly from the contralateral hemisphere)
mainly from the contralateral hemisphere)
4. Proximal, customarily symmetrical movements, such as chewing and swallowing, receive about the same number of UMN axons from each hemisphere, let us say 50/50.
5. The freest, independent unilateral movements are innervated by crossed and uncrossed UMN axons in a ratio of, let us say, 90/10. For movements with an intermediate degree of unilateral independence, the ratio might be 60:40, and so on.
6. Now predict the pattern of facial muscle weakness after unilateral destruction of one corticobulbar pathway. The Pt would show most paralysis of  forehead wrinkling/
forehead wrinkling/ eyelid closure/
eyelid closure/ lip retraction and least paralysis of
lip retraction and least paralysis of  forehead wrinkling/
forehead wrinkling/ eyelid closure/
eyelid closure/ lip retraction. (
lip retraction. ( lip retraction
lip retraction  forehead wrinkling)
forehead wrinkling)
7. Facial weakness after acute, severe interruption of UMNs
a. After a large, acute UMN lesion, such as a massive cerebral infarct, eyelid closure is usually paretic (incomplete paralysis), along with paralysis of lip retraction. Rarely, even the frontalis muscle is somewhat paretic. Because such a Pt has weakness of eyelid closure, the Ex who does not understand the gradient of unilaterality of facial movement may erroneously diagnose a lesion of the ipsilateral facial nerve rather than the contralateral corticobulbar tract.
b. In the acute phase, shortly after a severe UMN lesion, lip retraction contralateral to the lesion will be paralyzed during volitional movement and during emotional expression, such as smiling (Videos 6-4 and 6-5).

Video 6-4. Left upper motor neuron facial paresis associated with a left pronator drift.

Video 6-5. A child with left spastic hemiparesis secondary to a right internal carotid artery dissection. Note characteristic features of upper motor neuron (UMN) pattern of facial paralysis.
c. In the chronic phase of the UMN lesion, especially if the Pt has bilateral UMN lesions, lip retraction may remain weak during volitional action but may be prominent or even exaggerated during emotional expression (Monrad-Krohn phenomenon). See pseudobulbar palsy in Section VIII of this chapter.
D. Clinical testing of cranial nerve VII motor function
1. Facial inspection begins upon meeting the Pt and continues while taking the history.
a. Notice the overall play of facial muscles during speech and emotional expression. The face may move too much or too little. Many disorders, such as muscular dystrophy (Fig. 1-13I), parkinsonism, and depression, reduce all facial movements, a condition called masked facies, as if the Pt wore an immobile mask.
b. Excessive or involuntary movements seen on inspection of the face include blepharospasm, which may close the eyelids so tightly that the Pt cannot see; hemifacial spasm, in which all the muscles innervated by one of the VII nerves twitch; mass movements or synkinesis, whereby involuntary movements accompany a voluntary one (Peitersen, 2002); tics, chorea, and athetosis, as described in Chapter 7.
c. Next, search for asymmetry of facial movements, asymmetry of blinking, and asymmetry of the movement and depth of the nasolabial skin creases. The nasolabial creases begin just lateral to the lips and bow upward to the nares. To detect mild unilateral weakness of lip retraction after partial UMN lesions, watch for asymmetry of the depth and movement of these creases. Using your mirror, observe these two creases when your lips are at rest, when you smile, and when you speak (say EEE loudly). Slight congenital asymmetries are common.
2. Work through Table 6-1 with a partner. Often it is quicker to demonstrate the desired movements and give the commands. In working through Table 6-1, pay particular attention to the strength of eyelid closure. Can you open your partner’s eyelids against a maximum effort at closure?
_________
E. Analysis of patients with facial weakness
1. The Pts shown in Figs. 6-7 and 6-8 were asked to pull back the corners of their mouths, as in smiling, and simultaneously to close their eyes tightly. Make sure that you understand that the side that shows the action, that “draws to one side,” is the normal one. The side that fails to move is the abnormal one. The Pt with a facial palsy may state in the history that the face “draws to one side,” as if that were the abnormality. Especially compare both sides of each face for asymmetry of facial movement and for differences in the bulk of the chewing muscles.

FIGURE 6-7. Patient 1 with facial palsy. She was asked to close her eyes tightly and to pull back the corners of her mouth, as in smiling.
FIGURE 6-8. Patient 2 with facial palsy. She was asked to close her eyes tightly and to pull back the corners of her mouth, as in smiling.
2. Describe the abnormalities of the Pt in Fig. 6-7. Be sure that you start at the hair and systematically examine every facial contour and feature.
_________
_________
a. In Fig. 6-7 the Pt has weakness of eyelid closure on the left, as shown by lack of contraction of the orbicularis oculi muscle and absence of any “crow’s feet” wrinkles around the eye. The mouth retractors on the left are paralyzed. When this Pt looked up, the left half of her forehead failed to wrinkle. This pattern of total paralysis of all facial muscles on the left side implicates a lesion of the  right/
right/ left VII nerve or the
left VII nerve or the  right/
right/ left corticobulbar tract. (
left corticobulbar tract. ( left VII nerve)
left VII nerve)
b. The cognoscente of physical diagnosis will also have detected the hollowing of the Pt’s left temporal fossa and the concavity over the left masseter muscle, indicating atrophy of the chewing muscles and thus a lesion of CrN _____. (V)
c. If you missed this finding, remember that you must compare both halves of the body, specifically looking for just such asymmetries. The patient in Fig. 6-7 had undergone surgery to remove an acoustic nerve tumor, a neurinoma. The tumor, expanding in the cerebellopontine angle, had already destroyed CrNs V and VII, but full abduction of her left eye indicated sparing of CrN ________. (VI)
d. Did you also wonder about her very short hair? It was just growing back after having been shaved off for the operation.
e. This Pt was one of a minority who fail to show Bell phenomenon when attempting to close the eyelids. If Bell phenomenon had occurred, the eye would have turned _________
3. Describe the abnormalities of the Pt shown in Fig. 6-8.
_________
_________
a. In Fig. 6-8, the right side of the Pt’s mouth failed to retract, and eyelid closure on the right was weak, as shown by the wider exposure of the upper eyelid and lack of wrinkling around the right eye. This “crow’s feet” wrinkling on the normal side resulted from the purse-string, sphincter action of the orbicularis oculi muscle. When the Pt in Fig. 6-8 looked up, her forehead acted equally on both sides. Thus, on the right side of her face, the Pt had active forehead movements, weak eyelid closure, and paralysis of mouth retraction. This gradient of facial weakness on the right side of the Pt’s face indicates a lesion of the  right/
right/ left facial nerve or the
left facial nerve or the  right/
right/ left corticobulbar tract. (
left corticobulbar tract. ( left corticobulbar tract)
left corticobulbar tract)
b. The Pt shown in Fig. 6-8 had a UMN facial palsy after an occlusion of her left middle cerebral artery had caused infarction of her left cerebral hemisphere.
BIBLIOGRAPHY · Cranial Nerve VII
May M, Schaitkin BM. The Facial Nerve. 2nd ed. New York, NY: Thieme Medical Publishers; 1999.
Peitersen E. Bell’s palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol. 2002;549(Suppl.):4–30.
III. CRANIAL NERVE IX AND X MOTOR FUNCTIONS
A. Peripheral distribution of cranial nerves IX and X
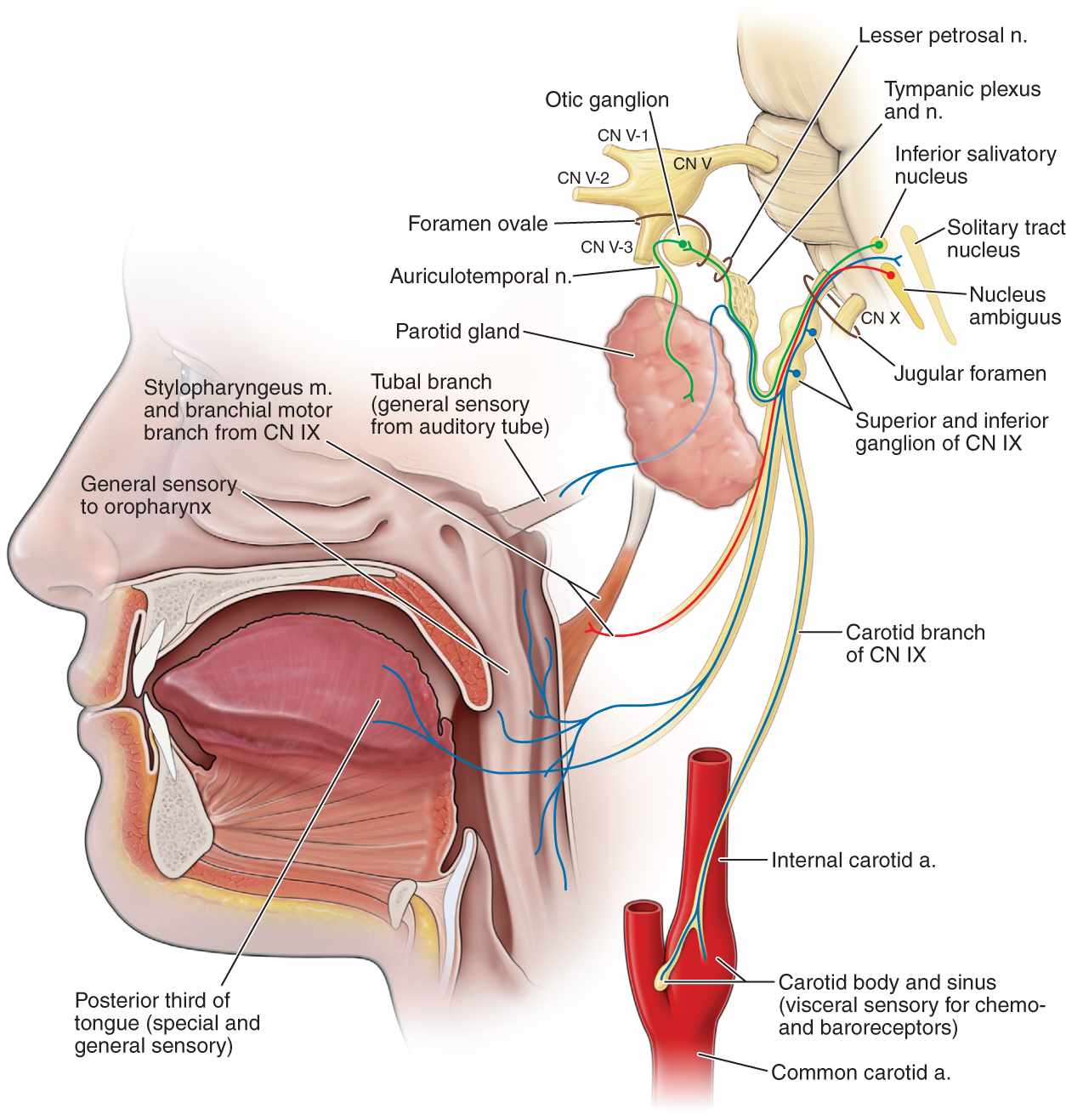
FIGURE 6-9. Innervation of the palate, tongue, and pharynx by cranial nerve IX. Motor axons innervate the stylopharyngeus and middle pharyngeal constrictor muscles. Sensory axons mediate taste from the tongue, the gag reflex, and the vasomotor, cardioinhibitory, and respiratory reflexes of the carotid body and sinus. (Reproduced with permission from Morton DA, Foreman K, Albertine KH. Chapter 17. Cranial Nerves. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.)
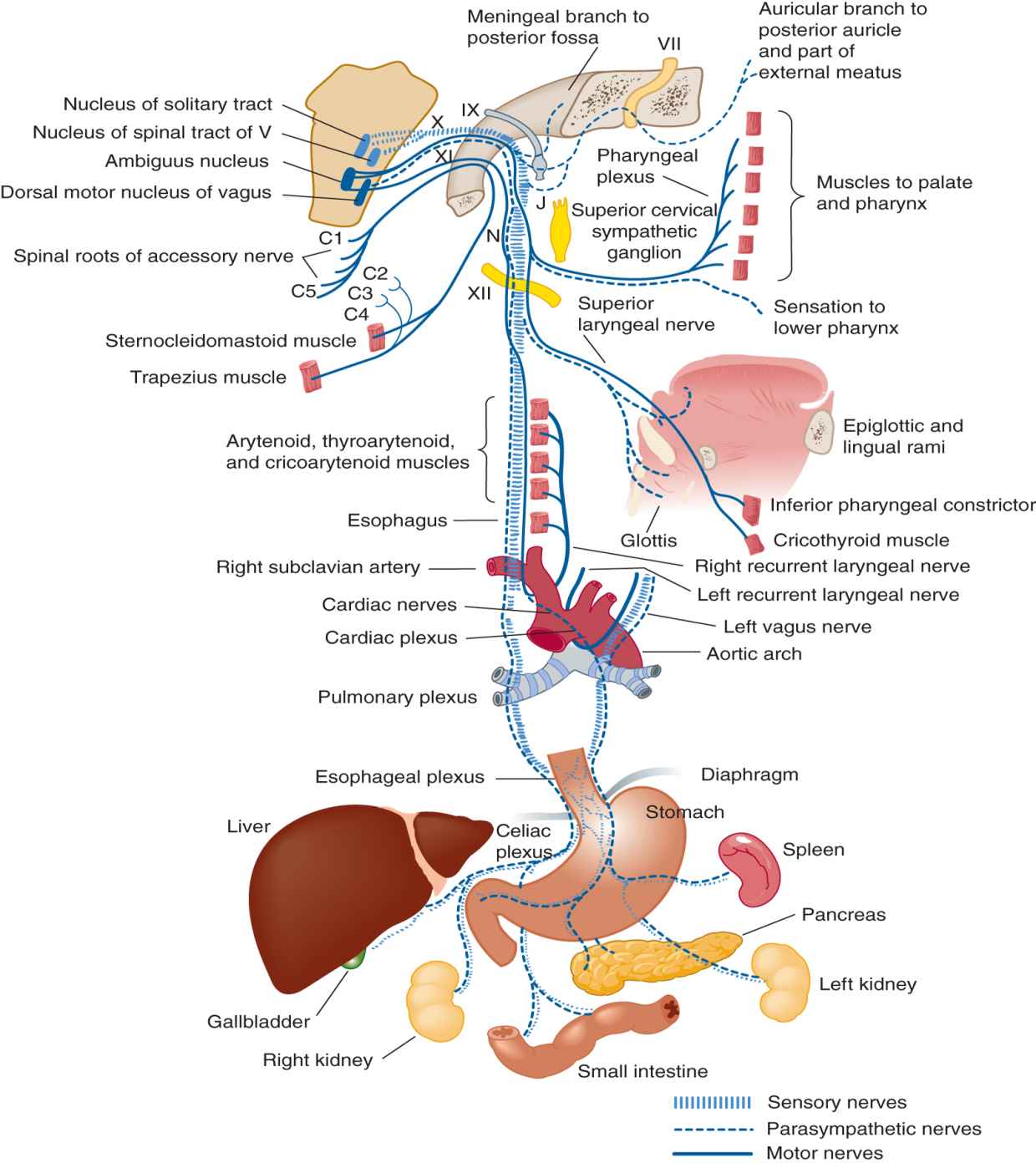
FIGURE 6-10. Innervation of the palate, pharynx, larynx, and thoracicoabdominal viscera by cranial nerve X. The palatal branch innervates the levator veli palatini muscle. The pharyngeal and laryngeal branches mediate sensory and motor functions of these structures. (Reproduced with permission from Waxman SG. Chapter 8. Cranial Nerves and Pathways. In: Waxman SG. eds. Clinical Neuroanatomy, 27e. New York, NY: McGraw-Hill; 2013.)
B. LMN innervation of the pharynx and larynx by cranial nerves IX and X
1. The skeletal muscles supplied by CrNs IX and X originally came from branchial arches. The branchial efferent nucleus for IX and X, the nucleus ambiguus, is in the  mesencephalon/
mesencephalon/ pons/
pons/ medulla. (
medulla. ( medulla (Fig. 2-14))
medulla (Fig. 2-14))
2. CrN IX supplies only one muscle exclusively (stylopharyngeus). Because this muscle aids in swallowing, its isolated function cannot be tested clinically. The remaining branchial efferent fibers of CrNs IX and X supply the pharyngeal constrictors. Because they act as a unit in swallowing, the isolated function of the individual constrictors cannot be tested at the bedside.
4. Because even complete interruption of CrN V has little clinical effect on palatal function, we can say that the motor functions of the palate, pharynx, and larynx are innervated by CrNs _______ and _______. (IX; X)
5. CrNs IX and X mediate sensation from the palate and pharynx and CrN X alone from the larynx. Hence, CrNs IX and X are the motor and sensory sentinels of the palatal orifice and pharynx, but CrN ___ alone is the sensorimotor nerve of the larynx. (X)
6. CrN IX also carries afferents from the carotid sinus that mediate baroceptive reflexes and from the carotid body that mediates baroceptive and chemoceptive reflexes.
C. Normal swallowing
1. Swallowing requires precise coordination of bulbar and respiratory muscles by a distributed network of neural connections involving the posterior inferior frontal gyrus, anterior insular region, basal motor nuclei, diencephalon, reticular formation, and cerebellum (Newton et al, 1994; Zald and Pardo, 1999). Lesions at various sites in this network may cause dysphagia (Groher, 1997). Unilateral lesions in the lowest part of the precentral gyrus and posterior part of the inferior frontal gyrus may impair swallowing without causing dysarthria (Wiles, 1991), although the two frequently coexist.
2. The tongue initiates the act of swallowing by voluntarily throwing a bolus of food back into the palatal archway. Tongue movements are innervated exclusively by CrN _____. (If you do not know, sort through CrNs I to XII to find the right one.) (XII)
3. Afferents from the palate via CrN IX then complete the act reflexly (Perlman and Schultze-Delrieu, 1997). The bolus stimulates the palate to elevate and deflect the bolus from the nasopharynx into the oropharynx. The pharyngeal constrictors contract, the larynx elevates, and the vocal cords close.
4. Swallowing requires afferent information via CrNs V, IX, and X, and motor actions are mediated by CrNs V, VII, IX, X, and XII. Connections in the region of the nucleus of the tractus solitarius in the medulla, in proximity to the respiratory center, act as a swallowing center. It coordinates the actions of swallowing and breathing to avoid aspiration (Newton et al, 1994; Smith Hammond, 2006); Section IV G describes clinical testing for disordered swallowing, ie, dysphagia).
5. Hold your jaw open and try to swallow with your lips open. You may succeed after a struggle, but normal swallowing requires sealing of the lips and closure of the jaw. CrN ___ innervates jaw closure and CrN ___ innervates lip closure. (V; VII)
D. Clinical physiology of the soft palate
1. The levator veli palatini muscle, innervated via the pharyngeal plexus by CrN X, swings the soft palate upward and backward to contact the posterior wall of the pharynx. This action seals off the naso pharynx from the oro pharynx. See Figs. 6-11A and 6-11B.
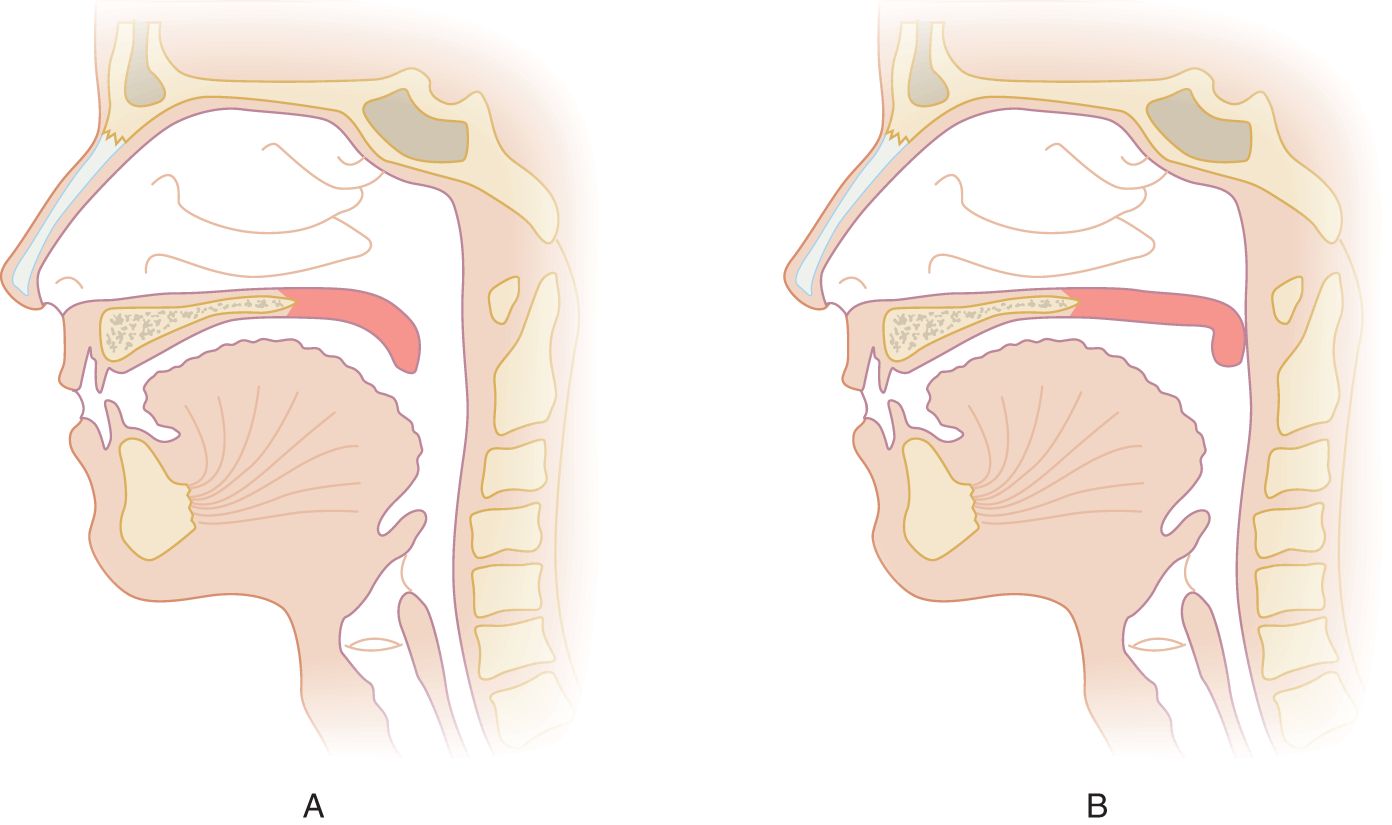
FIGURE 6-11. Sagittal section of the head. (A) Position of the soft palate when relaxed. (B) Position of the soft palate when elevated, occluding the nasopharynx from the oropharynx.
2. Unless the soft palate elevates properly, liquid will escape into your nose when you drink, and air will escape into your nose when you speak. The results are “nasal” swallowing and “nasal” speech. Because liquids and gases are fluids, we can agree that the soft palate and other branchial muscles of the throat control the fluid traffic at the oropharyngeal, nasopharyngeal, esophageal, and laryngotracheal openings. CrNs IX and X innervate, guard, and control the internal apertures of the head much as CrNs ____ (sensory) and ____ (motor) innervate the external apertures (eyes, mouth, ears, and nares). (V; VII)
3. The nasopharyngeal airway remains open until the palate elevates. The palate elevates as required to block anything in your oropharynx from entering your nasopharynx. Thus, the palate elevates when you:
a. Swallow
b. Whistle or trumpet
c. Make certain speech sounds
E. Upper motor neuron innervation of cranial nerves IX and X
1. The palate, pharynx, and vocal cords act with bilateral synchrony. By knowing this fact, you can predict that the number of crossed and uncrossed UMN fibers from each cerebral hemisphere would be about _________
2. Because of the usual bilateral UMN innervation, unilateral UMN lesions that cause hemiplegia only rarely cause unilateral weakness of the palate (Willoughby and Anderson, 1984), but Pts with acute hemiplegia frequently show mild dysarthria (about 60%).
BIBLIOGRAPHY · Cranial Nerves IX and X, Swallowing, and Dysphagia
Groher ME. Dysphagia: Diagnosis and Management. 3rd ed. Boston, MA: Butterworth Heinemann; 1997.
Newton HB, Newton C, Pearl D, et al. Swallowing assessment in primary brain tumor patients with dysarthria. Neurology. 1994;44:1927–1932.
Perlman AL, Schultze-Delrieu KS. Deglutition and Its Disorders: Anatomy, Physiology, Clinical Diagnosis, and Management. San Diego, CA: Singular Publishing Group; 1997.
Smith Hammond GA, Goldstein LB. Cough and aspiration of food and liquids due to oral-pharyngeal dysphagia ACCP evidence based guidelines. Chest. 2006;129(Suppl.):154S-N168S.
Wiles CM. Neurogenic dysphagia. J Neurol Neurosurg Psychiatry. 1991;57:1037–1039.
Willoughby EW, Anderson NE. Lower cranial nerve motor function in unilateral vascular lesions of the cerebral hemisphere. Br Med J. 1984;289:791–794.
Zald DH, Pardo JV. The functional neuroanatomy of swallowing. Ann Neurol. 1999;46:281–286.
IV. ROLE OF CRANIAL NERVES IN SPEECH
A. The basic physiology of speech
1. Speech requires a bellows, ergo lungs and respiratory muscles, that express a stream of air through the larynx and upper airway.
2. Speech requires a vibrator for phonation, ergo the vocal cords.
3. Speech requires articulation, ergo palate, tongue, lips, and mandible.
4. Speech requires resonance, ergo pharyngeal, oral, and nasal passages and cavities. The nasal passages resonate only three sounds of the English language: m, n, and ng.
5. Speech requires neural control, ergo UMNs to LMNs. Chapter 11 discusses cerebral circuits and cerebral disorders of speech.
B. Phonation: role of cranial nerve X
Galen (A.D. 130–200) of Pergamum was troubled by the squealing of piglets during surgical experiments. But his curiosity drove him to continue his investigations. Because he had no anesthetic, he eliminated the squealing and satisfied his curiosity with one stroke. After verifying the origin of the voice in the larynx, he found that he could silence it by cutting the recurrent laryngeal nerves, and that is how we learned what these nerves do.
C. Articulation of speech
1. Phonation versus articulation: After the larynx phonates, articulation shapes the sounds into speech. By whispering this sentence, you can clearly separate phonation from articulation. When whispering, you do not phonate at all, but you still articulate every word with perfect clarity. Articulate speech consists of a mixture of voiced and non-voiced sounds (Aronson, 1990).
2. Labial sounds: While watching your lips in a mirror, recite loudly each letter of the alphabet, but then try to repeat each letter without any lip movement. In Table 6-3, check the sounds that require strong labial action.
TABLE 6-3 • Letter Sounds Requiring Strong Lip Action (Labials)
Strong labial | Strong labial |
A | N |
B | O |
C | P |
D | Q |
E | R |
F | S |
G | T |
H | U |
I | V |
J | W |
K | X |
L | Y |
M | Z |
3. Lingual sounds: Complete Table 6-4 by reciting the alphabet loudly and checking the sounds that require strong lingual actions.
TABLE 6-4 • Letter Sounds Requiring Strong Tongue-Tip Elevation (Linguals)
Strong lingual | Strong lingual |
A | N |
B | O |
C | P |
D | Q |
E | R |
F | S |
G | T |
H | U |
I | V |
J | W |
K | X |
L | Y |
M | Z |
4. Vowel sounds
a. Compare the tongue actions when making D, G, and J sounds, strong linguals, with those needed to make the vowel sounds A, E, I, O, and U. To understand tongue action during vowel sounds, press down on your tongue with a tongue blade as you recite the vowels.
b. Vowels require palatal elevation. The palate does not completely seal off the nasopharynx during most speech sounds. Instead, it reduces the nasopharyngeal aperture, thereby detouring most of the air through the mouth, the path of least resistance. Only a few sounds require complete palatal closure:
i. Plosives: K or hard G, as in good.
ii. Vowels: sustained EEEEE… or Ah…
Related posts:
 A Synopsis of the Neurologic Investigation and a Formulary of Neurodiagnosis
Clinical and Laboratory Tests to Distinguish Conversion Disorder (Functional Neurologic Symptom Disorder) from Organic Disease
The Patient’s Mental Status and Higher Cerebral Functions
Examination of the Patient Who Has a Disorder of Consciousness
Examination of the Special Senses
Examination of the Somatic Motor System (Excluding Cranial Nerves)
A Synopsis of the Neurologic Investigation and a Formulary of Neurodiagnosis
Clinical and Laboratory Tests to Distinguish Conversion Disorder (Functional Neurologic Symptom Disorder) from Organic Disease
The Patient’s Mental Status and Higher Cerebral Functions
Examination of the Patient Who Has a Disorder of Consciousness
Examination of the Special Senses
Examination of the Somatic Motor System (Excluding Cranial Nerves)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


