Extradural Lesion, T2 Hyperintense, T1 Isointense
Bryson Borg, MD
DIFFERENTIAL DIAGNOSIS
Common
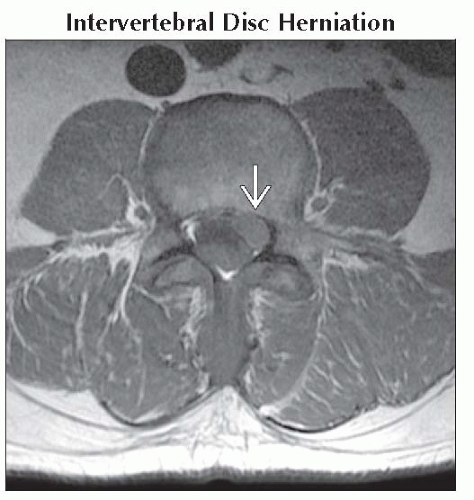
Intervertebral Disc Herniation
Synovial Cyst
Peridural Fibrosis
Epidural Fluid Collections
Abscess, Epidural
Hematoma, Epidural-Subdural (Acute)
Epidural Metastatic Disease
Neurofibroma
Schwannoma
Rare but Important
Primary Bone Tumor
Plasmacytoma
Lymphoma
Chordoma
Chondrosarcoma
Giant Cell Tumor
Ewing Sarcoma
ESSENTIAL INFORMATION
Helpful Clues for Common Diagnoses
Intervertebral Disc Herniation
Most common epidural lesion in adult population
Intermediate-to-low T1 signal
Variable T2 signal, depending on disc hydration
Herniations of the protrusion and extrusion subtypes most frequently hypointense relative to normal disc
Sequestered disc fragments often of moderate-to-high T2 signal
Synovial Cyst
Circumscribed, fluid-filled structure
Variable iso- or hypointensity on T1WI; centrally hyperintense on T2WI
Adjacent/contiguous with a facet joint
Cyst along ventral facet may impinge on thecal sac or nerve root
Seen with degenerative facet changes
Peridural Fibrosis
Epidural scar formation following spinal surgery
Normal post-operative finding
Infiltrative morphology, rarely mass-like
Isointense T1; variable T2 signal, usually hyperintense relative to disc material
May surround nerve root
Can only be differentiated from recurrent disc herniation on post-contrast imaging
Peridural fibrosis will homogeneously enhance, blending into extradural fat on non-FS T1WI
Abscess, Epidural
May be associated with disc space infection or instrumentation/direct inoculation
Contents typically approximate fluid signal on T1/T2WI
Increased T1 signal (isointense) may occur secondary to increased protein content
Marked peripheral enhancement typical on post-contrast imaging
Hematoma, Epidural-Subdural (Acute)
May be spontaneous or associated with trauma or instrumentation
Signal varies with the age of the hemorrhage
Acute hemorrhage (oxyhemoglobin) iso- or mildly hypointense on T1WI, hyperintense on T2WI
Minimal or no enhancement on post-contrast imaging
Epidural Metastatic Disease
Enhancing soft tissue mass, may be multiple
Most often associated with epidural extension from a vertebral metastasis
May also occur with transforaminal spread from a paraspinal or posterior mediastinal tumor
Neurofibroma
Enhancing nodular, fusiform, or dumbbell mass associated with a nerve root
Epidural neurofibroma typically intraforaminal or transforaminal
May be associated with vertebral scalloping, thinning/remodeling of pedicles
Most (90%) solitary, nonsyndromic
May be multiple, extensive; associated with plexiform neurofibromas (neurofibromatosis type 1)
Schwannoma
Helpful Clues for Rare Diagnoses
Plasmacytoma
Solitary plasma cell tumor, osteolytic tumor, ± compression fracture, ± extraosseous extension
Often indistinguishable from lytic metastases
Lymphoma
Enhancing epidural mass or epidural extension from a vertebral lesion
Often indistinguishable from metastases
Spinal lymphoma may also manifest with leptomeningeal or intramedullary lesions
Chordoma
Arises from notochord remnants: Midline, osteolytic tumor
Sacrococcygeal location most common, followed by clivus; vertebral lesion rather uncommon
May extend into epidural/paraspinal spaces
Heterogeneous iso- or hypointense on T1WI; marked hyperintensity on T2WI
Variable enhancement
Chondrosarcoma
Destructive tumor, chondroid matrix
Iso- or hypointense on T1WI; marked hyperintensity on T2WI
Heterogeneous enhancement
Giant Cell Tumor
Lytic, expansile vertebral body lesion; narrow zone of transition
May extend into epidural/paraspinal spaces
Heterogeneous iso- or hypointense on T1WI; heterogeneous hyperintensity on T2WI
Areas of low-to-intermediate T2 signal may reflect areas of high collagen content and hemosiderin deposition
Propensity to extend across sacroiliac joint & disc space is unusual for other lesions and may simulate infection
Ewing Sarcoma
Destructive tumor
Iso- or hypointense on T1WI; moderate to hyperintense signal on T2WI
Paraspinal soft tissue mass often a feature of spinal Ewing sarcoma
Image Gallery
 Axial T1WI MR shows sequestered disc fragment in the left anterolateral spinal canal
 . The fragment is similar in signal to skeletal muscle on T1WI. . The fragment is similar in signal to skeletal muscle on T1WI.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|