and Colin L. W. Driscoll2
(1)
Department of Otolaryngology – Head and Neck Surgery, Stanford University, Stanford, CA, USA
(2)
Department of Otorhinolaryngology, Mayo Medical School, Rochester, MN, USA
Concept
Nerve decompression is performed when the facial nerve is intact but inflamed. In this situation, the pressure within the fallopian canal increases above that of the mean arterial blood pressure, and the nerve becomes ischemic. This can lead to permanent facial nerve paresis or paralysis. Decompression treats this condition by removing the bony sheath covering the facial nerve. By achieving adequate decompression (i.e., at least 90° and more typically ~180° of the nerve’s circumference), a nerve that is inflamed and edematous can swell without having the pressure within the fallopian canal increase.
When the facial nerve is transected, primary nerve repair or interpositional nerve grafting are the preferred reconstructive options.
When the proximal end of the facial nerve is not accessible, facial reanimation can be achieved by connecting the distal end of the facial nerve to either CN V (trigeminal–facial anastomosis) or CN XII (hypoglossal–facial anastomosis).
Conditions treated
Facial nerve palsy due to Bell’s palsy with >90 % nerve degeneration diagnosed by ENoG can be treated by decompression.
Facial nerve palsy due to trauma such as a temporal bone fracture can be treated by decompression (if it is intact) or nerve repair or interpositional nerve grafting (if it is transected).
Facial nerve paralysis after resection of an invasive tumor.
Iatrogenic injury to the facial nerve.
Nerve decompression may be performed for facial nerve palsy due to compression by a cholesteatoma.
Risks
Poor facial function. Once the facial nerve has been divided, none of the reconstruction techniques provide better than a House–Brackmann grade 4/6 function.
Hearing loss
Benefits
Repair of the facial nerve provides dynamic motion to the face as opposed to static procedures that provide symmetry at rest but obvious asymmetry with motion.
1.
Illustration of the approach for facial nerve decompression in the mastoid. A postauricular incision is made.
2.
The soft tissues are reflected off the mastoid cortex.
3.
A simple cortical mastoidectomy is performed. The ear canal is thinned.
5.
The facial nerve can be found just inferior to the second genu, which is a highly consistent location. It is at the same depth in the mastoid as the lateral semicircular canal. The vertical segment can then be traced inferiorly to the stylomastoid foramen. By carefully thinning and removing the bone over the facial nerve epineurium (shown in the cases below), decompression is performed.
In order to access and decompress the horizontal segment of the facial nerve, the incudostapedial joint is separated, the incus and incudal buttress is removed, and the head of the malleus is clipped. This permits visualization of the horizontal facial nerve all the way to the geniculate ganglion (shown in the cases below).
In order to decompress the labyrinthine segment of the facial nerve, a middle fossa approach or translabyrinthine approach is used depending on whether a hearing preservation or nonhearing preservation strategy is desired.
6.
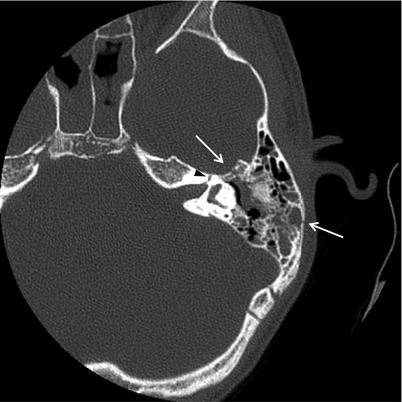
Case 1. Facial nerve decompression. Axial CT scan of a patient who sustained a left longitudinal temporal bone fracture and developed delayed-onset total facial nerve paralysis. The fracture line (arrows) went from the mastoid cortex to near the geniculate ganglion. Presumably, the facial nerve sustained a stretch injury in this location. ENoG testing revealed >90 % degeneration, and a total facial nerve decompression was performed. There is blood within the mastoid air cells. The labyrinthine portion of the facial nerve is visible (arrowhead). Decompression in this setting is controversial but may result in the best chance of satisfactory recovery. In addition, nerve repair can be performed if the nerve is found to have been transected.
7.
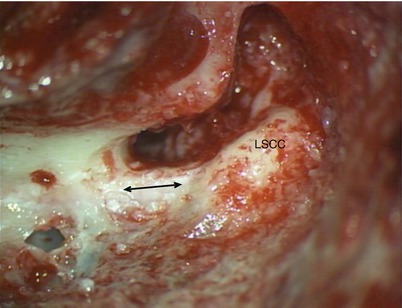
First, a standard canal wall up mastoidectomy was performed to decompress the horizontal and vertical segments of the facial nerve. The incudostapedial joint was divided, the incus removed, and the head of the malleus clipped. When approached through the mastoid, there is no way to access the horizontal segment without doing this. Often, the ossicular chain is already disrupted due to the fracture; if not, this portion of the nerve may be decompressed along with the geniculate ganglion and labyrinthine section through a middle fossa approach. The vertical segment of the facial nerve (arrow) is visible through the bone just inferior to the lateral semicircular canal (LSCC).
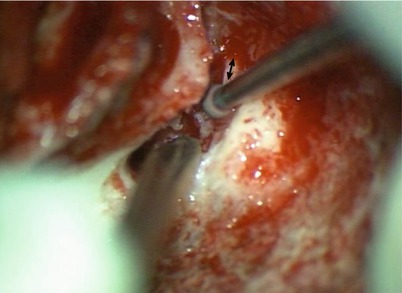
8.
The bone overlying the horizontal segment of the facial nerve (arrow) was carefully thinned with the drill.
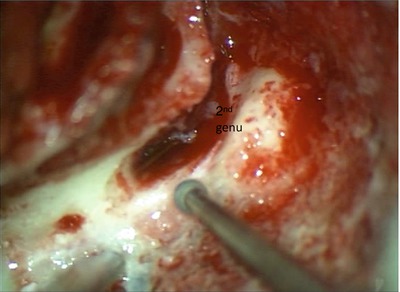
9.
The facial nerve was followed through the second genu.
10.
The vertical segment was followed inferiorly. This can be continued all the way to the stylomastoid foramen if desired. In this case, we did not because the injury was limited to the region near the geniculate ganglion.
11.
Once the bone overlying the nerve was thinned, it was removed manually (rather than with the drill) to minimize trauma to the nerve.
12.
The remaining thin fragments of bone over the horizontal segment were also picked away manually.
13.
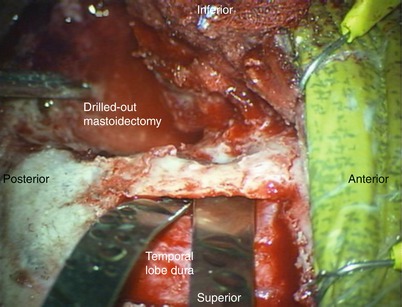
A middle fossa craniotomy was then performed. Note that viewing angle has changed because the surgeon has moved to the head of the bed. The malleable retractors were positioned within the extradural space, and the drilled-out mastoidectomy is visible.
14.
The temporal lobe dura was retracted to expose the floor of the middle cranial fossa.
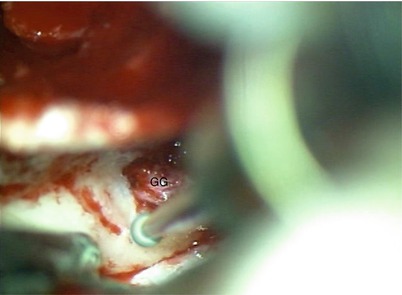
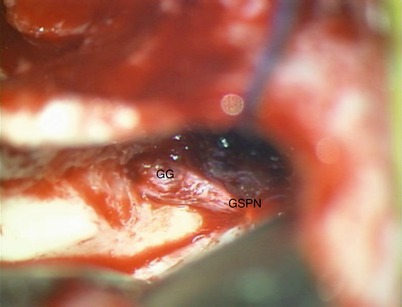
15.
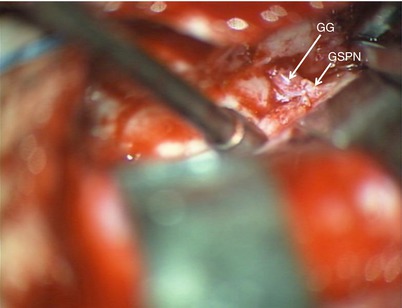
The geniculate ganglion (GG) was found to be dehiscent and quite swollen. The greater superficial petrosal nerve (GSPN) branched off anteriorly and was adherent to the dura as is typical.
16.
Drilling commenced medial to the geniculate ganglion (GG).
17.
After separating the GSPN from the dura for a short distance.
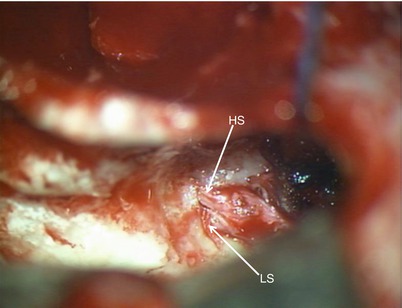
18.
Further drilling demonstrates the beginnings of the horizontal segment (HS) and the labyrinthine segment (LS) of the facial nerve.