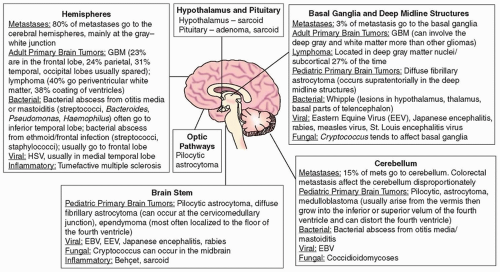
 FIGURE 17.1 Common causes of focal lesions in the brain based on location. GBM, glioblastoma; HSV, herpes simplex virus; EBV, Epstein-Barr virus. |
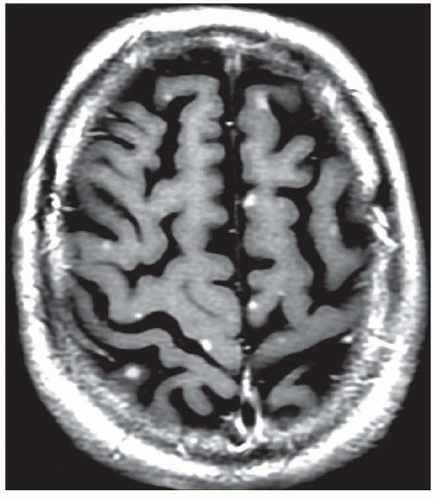 FIGURE 17.2 Metastatic small cell lung cancer. T1 MRI of the brain shows multiple small enhancing metastatic nodules. |
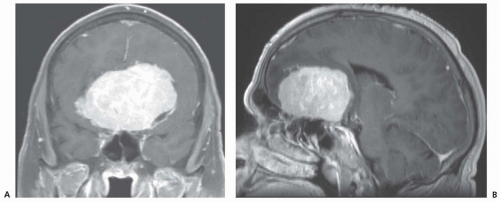 FIGURE 17.3 Large parasagittal olfactory groove meningioma strongly enhancing after contrast. Note the small cleft of CSF noted along the left margin of the lesion (coronal image, panel A). |
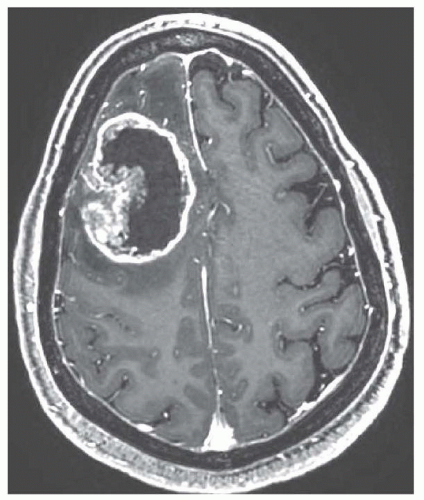 FIGURE 17.4 Glioblastoma multiforme. T1 MRI shows central necrosis and ring enhancement with a nodular component extending into the center of the lesion. |
adult primary brain tumors, in order of frequency, are pituitary adenomas (Fig. 17.6 and Chapter 100), nerve sheath tumors such as acoustic neuromas (see Chapter 102), and primary central nervous system (CNS) lymphomas (Fig. 17.7 and Chapter 99). Table 17.1 outlines typical clinical features, imaging findings, and suggested ancillary testing in adult patients with suspected brain neoplasm.
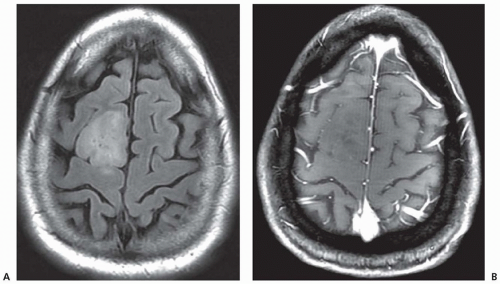 FIGURE 17.5 FLAIR (A) and T1 gadolinium enhanced (B) MR of a right frontal oligodendroglioma showing very little contrast enhancement and very little surrounding edema. |
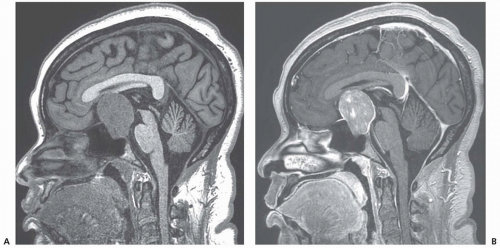 FIGURE 17.6 Pituitary macroadenoma. A: Hypointense on T1. B: Enhancing postcontrast. |
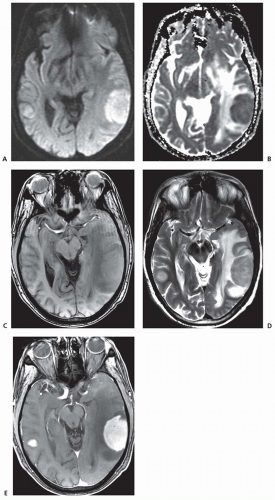 FIGURE 17.7 Primary CNS lymphoma. A: MRI restricted diffusion of DWI. B: Reduced apparent diffusion coefficient (ADC) appears as a dark core. C: T1 hypointense. D: T2 hyperintense peripherally due to edema tracking through the white matter. E: Avid contrast enhancement with gadolinium on T1 imaging. |
TABLE 17.1 Common Adult Brain Tumors | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||
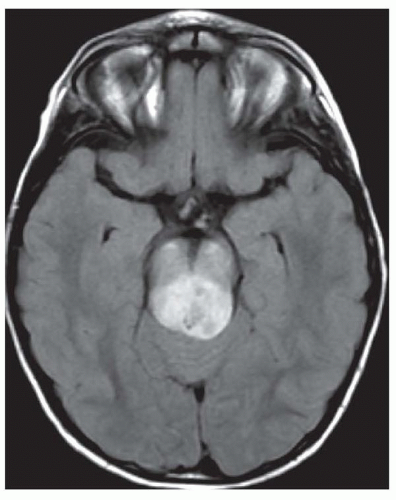 FIGURE 17.8 Pilocytic astrocytoma with high signal intensity on FLAIR imaging invading the midbrain. |
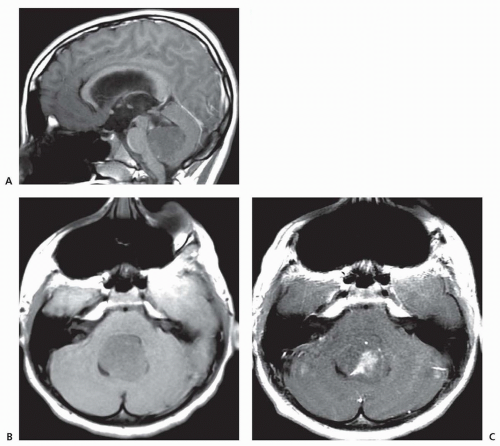 FIGURE 17.9 Medulloblastoma with distortion of the fourth ventricle and secondary hydrocephalus. A and B: Hypointense on T1. C: Moderate partial gadolinium enhancement. |
Coccidioides are most common in immunocompetent patients. The most common parasitic organisms that causes brain abscess are by far toxoplasmosis (Fig. 17.13) and cysticercosis (Fig. 17.14), although Strongyloides and Entamoeba histolytica are also common causes (see Chapter 65). Tuberculosis forms solid tuberculomas; after the caseous core liquefies, the tuberculoma becomes a tuberculous abscess (see Chapter 64). Syphilis can form gummas, cysticercosis can cause an inflammatory mass lesion when the cyst degenerates and dies, and viruses such as herpes simplex 1 (see Chapter 66) can cause encephalitis complicated by acute swelling and inflammation of the affected temporal lobes (Fig. 17.15).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


