13 Frontal Sinus Management in Skull Base Surgery
Kristin Seiberling and Peter-John Wormald
 Introduction
Introduction
The endonasal approach to skull base tumors requires a complete understanding of the endoscopic anatomy of the ventral skull base and surrounding structures. The anterior skull base consists of the frontal bone, fovea ethmoidalis, and intervening cribriform plates. Posteriorly the fovea ethmoidalis attaches to the planum sphenoidale. The first step in the removal of skull base tumors endonasally is complete clearance of the entire skull base. This is accomplished by performing a bilateral sphenoethmoidectomy followed by exposure of the frontal sinus. The surgical approach to the frontal sinus during the removal of skull base tumors depends on the extent and location of the lesion.
Prior to planning the surgery, the surgeon must review the preoperative images and evaluate the extent of the tumor along the parasagittal plane. Lesions located anteriorly along the skull base require maximum visualization of the frontal sinus and skull base, which necessitates a modified endoscopic Lothrop (MEL) procedure (Fig. 13.1A).
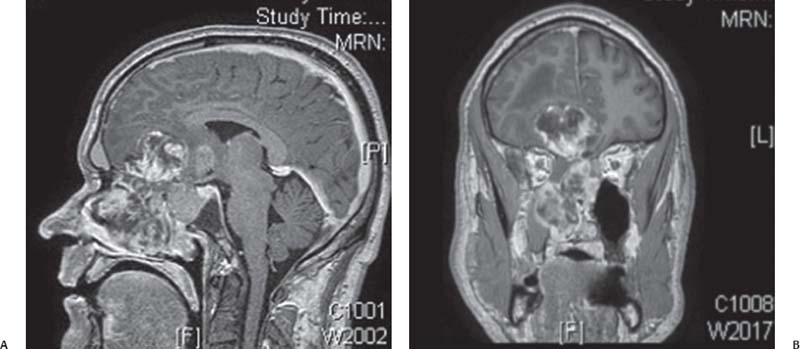
Fig. 13.1 Parasagittal (A) and coronal (B) magnetic resonance imaging (MRI) scans demonstrate a large T4 adenocarcinoma approaching the posterior table of the frontal sinus.
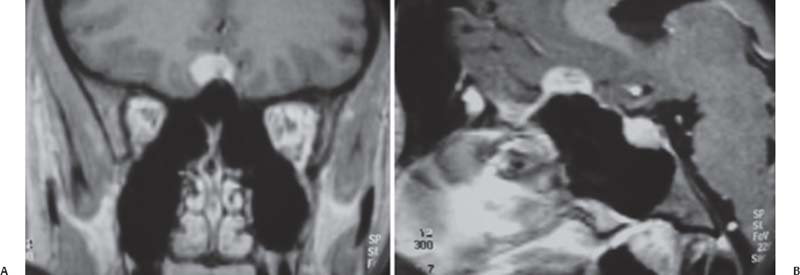
Fig. 13.2 Parasagittal (A) and coronal (B) MRI scans of a small posterior based meningioma.
Although each case must be individualized, it is thought that if the tumor approaches the region of the anterior ethmoidal artery, a MEL should be performed. The anterior ethmoidal artery is located between the frontal sinus ostium and upward continuation of the anterior face of the bulla ethmoidalis (Fig. 13.1B). The MEL facilitates accurate delineation of the skull base anteriorly at the level of the olfactory fossa. Lesions located in the posterior region of the anterior skull base may be removed with the identification of both frontal sinus ostia without a MEL (Fig. 13.2). If the tumor does not extend past the planum sphenoidale, identification of the frontal sinus ostia may not be necessary (Fig. 13.3).
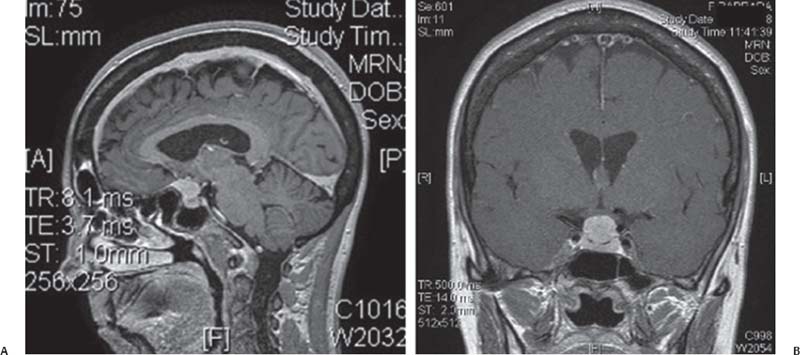
Fig. 13.3 Parasagittal (A) and coronal (B) MRI scans of a suprasellar meningioma. This tumor did not extend past the planum sphenoidale, which allowed for removal without dissection of the frontal recess.
 Surgical Anatomy
Surgical Anatomy
The frontal recess/sinus is a challenging area to approach surgically, given its proximity to the thin cribriform plate medially, the orbit laterally, and the anterior ethmoidal artery posteriorly. To access the frontal sinus, one must first understand the relationship of the drainage pathway of the frontal sinus to the surrounding structures.
In addition, to perform a MEL procedure, one must also grasp the relation of the frontal recess and frontal sinus to the frontal process of the maxilla, the nasal septum, the middle turbinate, the lacrimal sac, and the olfactory fossa. The thick bone of the frontal process of the maxilla, otherwise known as the frontal beak, forms the anterior wall of the frontal recess.
Anterior to the middle turbinate this bone continues to cover the lacrimal sac. The orbit is found posterior to the axilla of the middle turbinate. As long as the dissection is carried anterior or superior to the axilla, the orbit is not at risk. Another area of concern when drilling during a MEL procedure is the skull base in the region of the olfactory fossa.
To safely perform a MEL procedure one must have a strong grasp of the anatomy of the forward projection of the skull base, which forms the frontal T. The frontal T is located at a point where the middle turbinate attaches to the skull base at the anterior end of the olfactory fossa and marks the point of entry where the olfactory neurons are found. The olfactory neurons are a reliable marker for the level of the skull base used during the MEL procedure.
 Modified Endoscopic Lothrop (Draf 3 or Frontal Drillout)
Modified Endoscopic Lothrop (Draf 3 or Frontal Drillout)
The MEL procedure (also known as the Draf 3 or frontal sinus drillout) was originally described by Lothrop1 in 1914 and revised by Draf2 in 1991 and Gross et al3 in 1995. It involves the removal of the superior portion of the septum, the floor of the frontal sinus, and the intersinus septum, thus creating the largest possible opening between the frontal sinus and the nasal cavity (Fig. 13.4). This technique effectively exposes the posterior table of the frontal sinus and identifies the level of the skull base at its anteriormost extent.
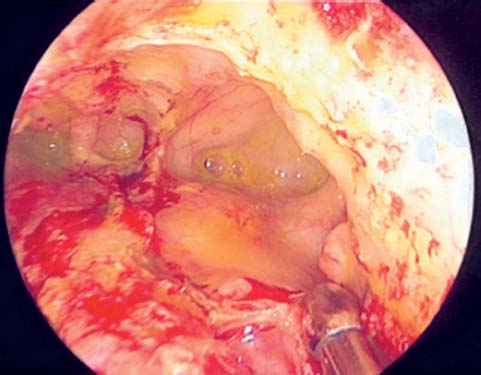
Fig. 13.4 Endoscopic view of the frontal sinus after a modified Lothrop.
In patients who have tumors that occupy the anterior skull base, a MEL is performed to delineate the level of the skull base anterior to the tumor. This enables the entire skull base to be skeletonized, facilitating tumor removal.
 Surgical Technique
Surgical Technique
Prior to starting the procedure, relevant CT scans are reviewed for the anatomy of the frontal recess and dimensions of the frontal sinus. A review of the axial, coronal, and parasagittal scans is necessary to determine the anatomy and outflow tract of the frontal sinus. Image guidance is setup and used during the procedure. We routinely use image guidance in all our MEL and skull base procedures. Image guidance enables confirmation of the position of the first olfactory neurons, which mark the level of the skull base in the region of the olfactory fossa.
The surgery is begun with a zero-degree endoscope that is used for the majority of the procedure. This is switched to a 30-degree scope only at the end of the procedure when the frontal beak is taken down. The nasal septum, the region of the axilla of the middle turbinate and nasal vault, is injected with local anesthetic.
Using a powered microdebrider the mucosa over the frontal process of the maxilla superior and lateral to the axilla of the middle turbinate is removed up to the roof of the nose. Subsequently a 2 × 3 cm septal window is created, enabling instruments to be used from both sides of the nose, facilitating the dissection.
The posterior landmark for the septal window is the anterior edge of the middle turbinate (Fig. 13.5). The septal window is widened superiorly to the roof of the nose and inferior to the point where instruments may be passed easily from one side of the nose to the other. The surgeon must be able to place instruments through the septal window and under the axilla of the contralateral middle turbinate. Anteriorly, the septum is removed until both middle turbinates, the axilla, and the frontal process of the maxilla are clearly visualized (Fig. 13.6).
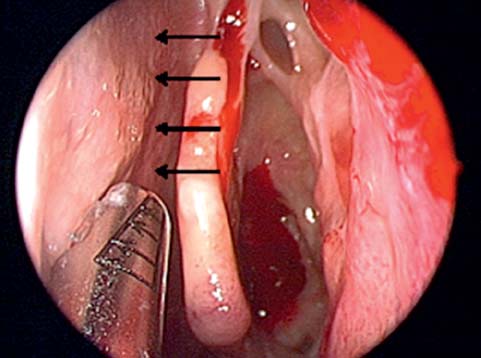
Fig. 13.5 The posterior edge of the septal window begins at the anterior edge of the middle turbinate (black arrows).
Related posts:
 Anesthesia in Endoscopic Skull Base and Brain Surgery
The Endonasal Transplanum-Transtuberculum Endoscopic Approach in Pituitary Adenomas
Endoscopic Transnasal Craniectomy and the Resection of Extensive Craniopharyngiomas
External Versus Endoscopic Approaches for Skull Base Malignancies
Pterygopalatine and Infratemporal Fossae
Anatomy of the Orbit and Related Structures
Anesthesia in Endoscopic Skull Base and Brain Surgery
The Endonasal Transplanum-Transtuberculum Endoscopic Approach in Pituitary Adenomas
Endoscopic Transnasal Craniectomy and the Resection of Extensive Craniopharyngiomas
External Versus Endoscopic Approaches for Skull Base Malignancies
Pterygopalatine and Infratemporal Fossae
Anatomy of the Orbit and Related Structures



