The evolution of locomotion has been very important for humans, as it enabled us to travel greater distances and interact with novel and complex environments. Bipedal locomotion also facilitated the evolution of complex manipulation skills. The capacity for independent gait is crucial for function: For instance, the loss of independent ambulation is a predictor of the need for long-term care in a number of age-related neurologic disorders. In addition to independent gait, achieving a requisite speed is also important for independent mobility in the community. For example, in people who have suffered a stroke, speed of 0.85 m/s is predictive of the ability to independently ambulate in the community.
Gait impairments are very common sequelae of aging and neurologic disorders. At the age of 60 years, about 15% people have gait impairments. Among people older than the age of 85 years, approximately 80% report gait impairments. Even among middle-aged individuals, approximately 40% report mild difficulties with mobility functions. Gait impairments can have devastating consequences, such as falls and injury. Approximately one-third of community-dwelling individuals older than the age of 65 years fall and fall-related injuries increase with age. An unfortunate consequence of gait impairments is that individuals often reduce their mobility in order to prevent falls and related incidents. However, reduced mobility further increases risk for falls by reducing muscle strength and worsening balance.
The purpose of this chapter is to briefly describe the gait cycle, the neural pathways underlying gait, the most commonly seen disorders of gait, and methods for clinical assessment of gait. Finally, we present the risk factors and assessment of falls in the elderly.
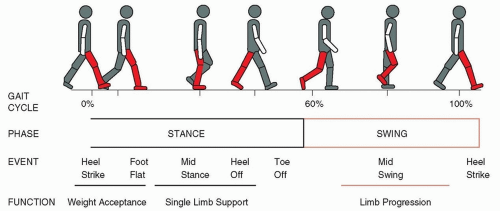
FIGURE 14.1 The gait cycle. The position of the right leg (shaded red) shows major events within the gait cycle during stance and swing phases.
INTRODUCTION TO THE GAIT CYCLE
The gait cycle consists of repetitive sequential movements of the limbs that help propel the body forward along a predetermined line of progression. The gait cycle is defined by foot contact with the ground and extends from the heel strike of one lower limb to the subsequent heel strike of the same limb (Fig. 14.1). We define two phases within each gait cycle: a stance phase, which consists of approximately 60% of the gait cycle and a swing phase, which consists of approximately 40% of the gait cycle. Stance phase begins with heel strike and ends with toe off and consists of three events—foot flat, midstance, and heel off. The function of the stance phase is to accept the weight of the body on to the supporting (stance) limb. At the beginning of stance (from heel strike to foot flat on the right side) and at the end of stance (from heel off to toe off on the right), both feet are on the ground simultaneously. The period of double support comprises approximately 20% of the gait cycle. During midstance, body weight is supported by one limb (single limb support). During a typical gait cycle, the lower limbs move in a symmetric alternating movement with a phase lag of 0.5 (indicating that when one limb initiates swing, the opposite limb is in the middle of stance phase).
The swing phase of a limb begins with toe off and ends with heel strike. The events within the swing phase (foot clearance and midswing) serve to allow the foot to clear the floor as it propels the body forward in preparation for the subsequent step. The events within the gait cycle described earlier pertain to walking at a comfortable preferred speed. As speed of gait increases, the percentage of time spent in double support decreases. During running, there is no double support phase. Gait can be described quantitatively with respect to its spatial and temporal features. Gait measures that can be assessed in the clinical setting are described in Table 14.1 and Figure 14.2.
TABLE 14.1 Definition of Clinical Gait Measures
Gait Variable
Definition
Speed
Distance covered in unit time (e.g., meters per second)
Cadence
Step frequency—number of steps in a given time (steps per minute)
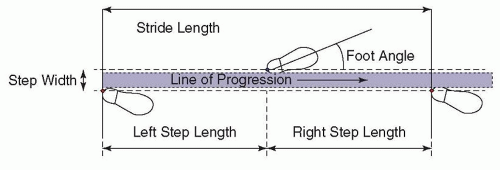
Step length
Distance (measured in meters along the line of progression) between successive heel strikes of the lower limbs
Stride length
Distance (measured in meters along the line of progression) between successive heel strikes of the same limb
Step width
Distance (measured in meters perpendicular to the line of progression) between successive heel strikes of the lower limbs
Step height
Vertical clearance of the foot from the floor during swing
Step symmetry
Ratio of step length on the right and left sides
Step continuity
Ratio of step time on the right and left sides
Foot angle
Angle formed by the long axis of the foot with the line of progression
Walking path
Direction of the line of progression
NEURAL CONTROL OF GAIT
Gait is a complex task that requires the coordinated activity of several brain circuits. Even walking in an uncluttered environment at a preferred speed (considered an easy task) elicits activity in higher cortical regions. The following description briefly discusses the role of different circuits in controlling gait. Readers interested in additional details are referred to excellent recent reviews in the suggested readings list. In order to successfully initiate and control gait, the nervous system needs to perform the following tasks:
Maintain balance against the force of gravity under static (e.g., during stance) and dynamic conditions (e.g., during walking). Maintenance of balance under dynamic conditions includes predictive and reactive control of destabilizing forces that are either generated internally (e.g., destabilizing forces generated by movement of the arms) or externally (e.g., destabilizing forces generated by bumping into another person).
Coordinate movements of the lower limbs to propel the body forward.
Help navigate complex environments, which may include stationary obstacles (e.g., furniture) and moving obstacles (e.g., people walking).
Perform concurrent tasks with walking, such as talking, listening, or manipulating objects (e.g., mobile phone).
FIGURE 14.2 Spatial characteristics of gait. Spatial gait variables defined by foot placement along the line of progression.
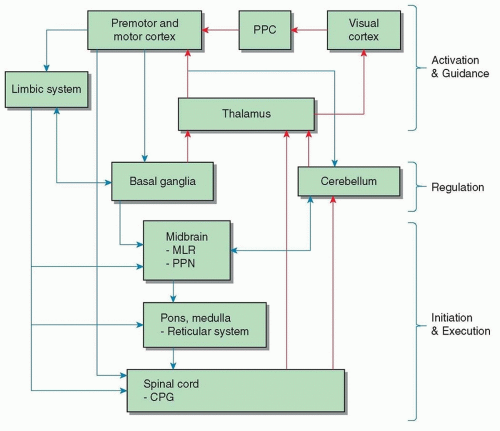
Most of the experimental work in understanding the neural control of gait has come from experiments with quadruped and biped animals. These experiments suggest that distinct neural circuits perform specific functions. Cortical circuits (including premotor and motor areas, parietal and occipital areas) are involved with activation and guidance. Reciprocal circuits between the cortex-basal ganglia and cortex-cerebellum are involved with regulation of gait (including postural tone, balance, and coordination of limb movement). Finally, brain stem and spinal cord circuits are involved with the execution of gait (including gait initiation, step frequency, reciprocal movements of the lower limbs). A simplified diagram of the neural structures involved in control of gait is presented in Figure 14.3 and functions of brain structures are summarized in Table 14.2.
ACTIVATION AND VISUAL GUIDANCE OF GAIT
Gait can be activated either by a volitional process under the control of cerebral cortical circuits or by emotional cues (fight or flight reaction) under the control of limbic circuits. Volitional guidance of gait requires precise visual information about the environment, which is processed in the visual areas of the occipital cortex. The posterior parietal cortex (PPC) receives information from the visual cortex and project to the motor areas in the frontal cortex. An important function of the PPC is to construct maps of space, which are very important for visual guidance of locomotion. The premotor areas, in particular the supplementary motor area (SMA), are important for postural control during gait. The motor cortex projects to interneurons and motor neurons in the spinal cord and is important in the control of limb movements during gait.
REGULATION OF GAIT
The basal ganglia and cerebellum have a major influence on motor output even though they do not directly project to the spinal cord. The basal ganglia input nuclei, in particular the putamen, receive inputs from the premotor and motor cortex. The output nuclei of the basal ganglia (globus pallidus internal segment and substantia nigra pars reticulata) project back to the premotor and motor cortex via the thalamus. These projections are thought to be important for regulating movement amplitude and speed. In addition, the basal ganglia send inhibitory projections to the midbrain locomotor region (MLR) and the pedunculopontine nucleus (PPN). The projection from the basal ganglia to the MLR is responsible for regulating the rhythmic aspects of gait. When there is damage to these projections, as seen in Parkinson disease and Huntington disease, rhythmic control of gait is impaired. The projection from the basal ganglia to the PPN is responsible for regulating muscle tone. Damage to these projections lead to disorders of postural muscle tone, as seen in Parkinson disease.
FIGURE 14.3 Neural control of gait. Schematic illustration of neural structures involved in the control of gait. Efferent connections are shown in blue arrows and afferent connections in red arrows. PPC, posterior parietal cortex; MLR, midbrain locomotor region; PPN, pedunculopontine nucleus; CPG, central pattern generator.
The cerebellum receives a tremendous amount of afferent information from the limbs and vestibular apparatus. In addition, projections from the cerebral cortex to the cerebellum provide information regarding the upcoming movement. The output of the cerebellum is directed to the motor areas of the cerebral cortex, midbrain (MLR and PPN), and brain stem (vestibular and reticular nuclei). A major function of the cerebellum is to evaluate disparities between intended movement and actual movement (based on feedback). The cerebellum is important for regulating balance and limb coordination during gait and for providing adaptability to novel conditions based on trial and error learning.
Two areas in the brain stem are important for initiating and executing locomotion—the MLR and the PPN. The MLR receives inputs from the cerebral cortex, limbic system, basal ganglia, and cerebellum. A primary function of the MLR is activation of spinal cord circuitry to initiate gait. Inputs from the motor areas and the limbic system to MLR provide the neural substrate for activation of gait based on volitional (motor areas) and emotional (limbic system) cues. The PPN also receives inputs from the motor areas of the cerebral cortex, limbic system, basal ganglia, and cerebellum. The PPN inhibits spinal interneurons and motor neurons. A major function of the PPN is to modulate muscle tone during stance and gait. The spinal cord circuitry includes networks of interneurons (central pattern generators) and motor neurons that innervate skeletal muscles. There are two sets of interneurons, termed half centers, that project to flexor and extensor motor neurons. The half centers mutually inhibit each other and are responsible for producing the basic locomotor pattern. Although the half centers do not require sensory input to generate the basic locomotor pattern, their activity can be modulated by sensory input from the limbs. For example, signals from proprioceptors of the hip flexors may be used to signal the end of stance phase. In addition, skin afferents from the limbs are important for adjusting stepping movements in the presence of obstacles. Thus, the function of the spinal cord is to execute the rhythmic movement pattern of gait.
DISORDERS OF GAIT
In neurologic disorders, gait performance is classified as disordered based on comparison with healthy subjects, for whom normative values through the course of aging are available. However, given the large variability of what is considered “normal” gait, caution must be used in order to describe gait patterns as impaired. Table 14.3 highlights gait impairments that are clinically evident in neurologic disorders. Several classifications have been proposed for gait disorders including anatomic, hierarchical (e.g., low, mid, and high level), etiologic (e.g., degenerative) or phenomenologic (e.g., antalgic gait). Anatomic classification describes gait disorders based on brain pathology (e.g., cerebellar gait). Hierarchical classification differentiates gait disorders into three categories based on the level of pathology (e.g., low level, midlevel, and high level). Gait disorders due to peripheral sensory (e.g., sensory ataxic) or motor disorders (e.g., spinal muscular atrophy) are classified as low-level disorders. Disorders that occur as a result of pathology in the motor system, including motor cortical areas, basal ganglia, and cerebellum, are classified as midlevel disorders. Finally, gait disorders that result from the interaction of cognitive (frontal cortex) and motor systems (e.g., Alzheimer disease) are classified as high-level disorders. Finally, classification of gait disorders by phenomenology takes into account etiology and clinical features. In this chapter, gait disorders are classified by hierarchy and pathophysiology, which more closely reflects clinical practice. The table also separates phenomena that may be observed throughout gait observation (continuous) from those that are unpredictable (episodic). According to this classification, continuous phenomena reflect the underlying pathology and compensatory mechanisms, whereas episodic phenomena are those that the patient cannot adapt to because of their unpredictability.
FALLS IN THE ELDERLY
Falls are defined as “unexpected events in which a person comes to rest on the floor, ground, or supporting surface.” Falls are considered an inevitable consequence of aging and may result in serious adverse events in older adults. Approximately one-third of community-dwelling people older than the age of 65 years fall each year. The number of falls is much higher for older people living in nursing homes: approximately 1.5 falls per bed per year. The high incidence of falls coupled with the susceptibility to injury (because of comorbidities and age-related physiologic changes) leads to adverse events in the elderly. Falls may result in injuries such as abrasions, bruising, lacerations, and sprains. It is important to note that falls resulting in minor injuries may be underreported by patients. A careful ascertainment of history of falls is very important in clinical practice. About 10% of falls result in fractures, the type of fracture depending on the nature of the fall. Forward or backward falls on outstretched hands result in wrist fractures, falls to the side result in hip fractures, and falls resulting in impact to the head may result in head injury and loss of consciousness. Backward falls on the buttocks result in lower rates of fractures, although fractures of the vertebrae can occur.
Falls account for two-thirds of accidental deaths. The other negative consequences of falls include increased fear of falls and reduced mobility. This results in a negative spiral: Reduced mobility leads to reduction in muscle strength, flexibility and postural stability, and gait impairments, all of which, in turn, increase the risk for additional falls. Falls have a significant negative impact on the quality of life of elders.
Risk factors for falls can be classified as intrinsic or extrinsic. Intrinsic factors include age, muscle strength, gait and balance impairments, and neurologic or cognitive disorder. Extrinsic factors include medications, environmental hazards, and type of activity (based on hazard). The greatest risk factors for falls are previous history of falls, muscle weakness, gait and balance impairments, use of walking aids, vertigo, Parkinson disease, and medication use. It is important to note that a number of these factors, such as weakness, gait and balance impairments, use of walking aids, and medications are modifiable factors. Often, patients report near falls, defined as a “loss of balance that would have resulted in a fall if sufficient recovery mechanisms (movement of the trunk or arms, change in stride length or velocity) were not activated.” Near falls often precede falls and are more frequent than falls. Clinical assessment of falls should include information on near fall events. More information on fall assessment appears in the following section. Physical exercise (under the supervision of a physical or occupational therapist) is effective in reducing the frequency of falls and preventing future falls. In addition, home hazard assessment and reduction (under the supervision of occupational therapists) reduces the frequency of fallers and the number of falls. Clinicians should consult physical and occupational therapists, as needed.
Only gold members can continue reading. Log In or Register to continue