Headache is one of the most frequent reasons for which patients seek medical attention and accounts for more disability on a global scale than any other neurologic problem when including direct and indirect costs. The appropriate management of headache disorders relies on a careful diagnostic approach that is based on an understanding of the physiologic mechanisms of head pain and different characteristics of both primary and secondary headache syndromes.
GENERAL PRINCIPLES
A classification system for headache disorders has been established by the International Headache Society (IHS). The most recent version, International Classification of Headache Disorders, 3rd edition, beta version (ICHD-3 beta) divides headache disorders into primary syndromes (in which the headache and associated features constitute the disorder itself) and secondary disorders (in which the headache results from exogenous causes).
The most common primary headache syndrome is tension headache comprising 69% of all primary headaches; however, such headaches are rarely debilitating and are generally self-treated with over-the-counter medications. The second most common primary headache disorder is migraine, with a 1-year prevalence of 12% (17% among women and 6% among men peaking around the fourth decade of life). Recurrent and disabling headaches in a primary care setting are most often migraines. Life-threatening headache is infrequent; however, caution and adequate surveillance are needed to properly diagnose and manage these cases.
DIAGNOSIS
The key to the proper diagnosis of headache is obtaining a comprehensive and precise history. Important components of the headache history include the following:
Onset: abrupt versus insidious; context in which headache began (e.g., recent head trauma, including head/neck surgeries, viral illness, pregnancy/postpartum)
Timing: chronicity, duration, and frequency of headache attacks; time to maximal intensity; diurnal versus nocturnal
Quality: for example, sharp, dull, pressure, throbbing, stabbing, lancinating, burning
Laterality: unilateral versus bilateral; side-locked versus alternating
Location: for example, retroorbital, frontal, temporal, occipital
Severity: including disability and interference with work/normal activities
Change: different pattern from prior headaches
Associated symptoms: sensory hypersensitivity (e.g., to light, noise, sound, smell, movement); nausea/vomiting; visual changes; numbness/tingling of the face or extremities; focal motor weakness; impairment of speech; light-headedness/vertigo; cognitive dysfunction
Cranial autonomic features: lacrimation, conjunctival injection, periorbital or facial edema, ptosis, pupillary changes; nasal congestion or rhinorrhea; aural fullness or tinnitus
Premonitory features: symptoms that are experienced days to hours prior to headache attacks (such as yawning, sleepiness, increased thirst, changes in bowel/bladder pattern, neck stiffness)
Triggers: for example, menstrual cycle; skipping meals; lack of sleep or oversleeping; stress or relaxation from stress; altitude or barometric changes; position (lying down vs. standing up); Valsalva maneuvers or physical exertion; bright lights, noise, or smells; alcohol; caffeine; and certain foods (such as those containing nitrates or monosodium glutamate)
Family history of headache disorders
Past medical history, review of systems, social history, concomitant medications, prior imaging, and labwork should also be reviewed in detail, as these may reveal an underlying cause for the headache.
The physical examination should include a comprehensive systemic and neurologic examination with particular attention to the following: bruits of the head or neck, temporal artery tenderness and pulsations, occipital nerve tenderness, pupillary size and symmetry, funduscopic examination (for evaluation of papilledema and retinal venous pulsations), visual field testing and extraocular movements, facial sensation (including corneal responses), and motor function.
The first goal of diagnosis is to differentiate between a benign headache disorder (usually a primary syndrome) and a serious underlying condition (secondary headache). There are a few tools available to help identify a potential life-threatening headache (using so-called red flags); conversely, the presence of “white or green flags” can suggest a more benign scenario.
RED FLAGS
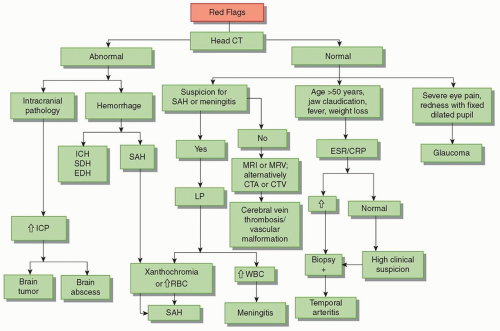
Symptoms that may point to a serious underlying disorder can be evaluated by the mnemonic “SNOOP” (Table 7.1). Despite the use of SNOOP, the neurologic examination remains the best predictor of structural intracranial pathology. The evaluation of a patient with headache in the emergency room is shown in Figure 7.1.
Alarming causes of secondary headaches that require urgent evaluation include meningitis, intracranial hemorrhage, acute ischemic event, tumor or obstructive lesion, glaucoma, purulent sinusitis, cortical vein/cranial sinus thrombosis, carotid/vertebral artery dissection, pituitary apoplexy, posterior reversible encephalopathy syndrome (PRES), and reversible cerebral vasoconstriction syndrome (RCVS). Patients who had a recent ischemic infarct and develop new-onset headache should also undergo immediate head computed tomography (CT) to rule out hemorrhage, particularly those patients who received thrombolysis. Thyroid disorders (most commonly hypothyroidism) are also frequently associated with headache.
TABLE 7.1 “Red Flags” When Evaluating Headache Symptoms
Systemic
Systemic signs/symptoms: stiff neck, vomiting preceding the headache, fever, night sweats, rash, myalgia, weight loss; also headache during pregnancy or postpartum and comorbid systemic disease (e.g., HIV, malignancy)
Neurologic symptoms
Change in mental status or level of consciousness; papilledema, diplopia; loss of sensation; weakness; ataxia; local tenderness (region of temporal artery); headache induced by Valsalva maneuvers (bending, lifting, cough, sneezing); pain that disturbs sleep or presents immediately upon awakening; history of seizure/collapse/loss of consciousness
Older
Onset after age 50 years
Onset
Onset sudden and/or first ever; severe or “worst” headache of life; “thunderclap” headache (pain reaches maximal intensity in an instant)
Pattern change
Change in frequency, severity, or clinical features of the attack; subacute worsening over days/weeks or accelerating pattern, continuous or persistent headache; pain triggered by sexual activity, Valsalva maneuver, or sleep; worsening with change in position
Adapted from Silberstein SD, Lipton RB, Dodick D, et al. Wolff’s Headache and Other Head Pain. 8th ed. New York: Oxford University Press; 2008.
FIGURE 7.1 Evaluation of a patient with headache in the emergency room. CT, computed tomography; SAH, subarachnoid hemorrhage; ICH, intracerebral hemorrhage; SDH, subdural hemorrhage; EDH, extradural hemorrhage; LP, lumbar puncture; MRI, magnetic resonance imaging; MRV, magnetic resonance venography; CTA, computed tomography angiography; CTV, computed tomography venography; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; ICP, intracranial pressure; RBC, red blood cell; WBC, white blood cell. (Adapted from Gordon DL. Approach to the patient with acute headache. In: Biller J, ed. Practical Neurology. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2012:194-206.)
TABLE 7.2 POUND Mnemonic for Identifying Migraine Headache
Pulsatile quality of headache
One-day duration (4-72 h)
Unilateral location
Nausea or vomiting
Disabling intensity
GREEN FLAGS
Certain clinical features support a benign primary headache disorder. Simple tools that can help identify migraine include ID Migraine, a set of three questions regarding photophobia, nausea, and disability simplified as “PIN” (photophobia, inability to function, and nausea). If two out of the three features are present, a diagnosis of migraine is likely (with sensitivity of 81% and specificity of 75%). If all three are present, there is a 93% probability of meeting IHS diagnostic criteria for migraine. Another tool is the POUND mnemonic (Table 7.2), in which the presence of four out of five features can accurately predict a diagnosis of migraine.
Despite present guideline recommendations, many clinicians overorder imaging in benign scenarios. The American Headache Society (AHS) created the “Choosing Wisely” recommendations to address the need for neuroimaging as follows:
No need for imaging in patients with stable headache that meet migraine criteria
No CT for headache when magnetic resonance imaging (MRI) is available except in emergency settings.
SECONDARY CAUSES OF HEADACHE
MENINGITIS
Presence of fever, stiff neck, and Kernig and Brudzinski signs (poor sensitivity but good specificity) warrant further workup with imaging (CT/MRI) followed by lumbar puncture for cerebrospinal fluid (CSF) analysis to rule out an infectious or inflammatory meningitis. If suspecting meningitis, cover with empiric antibiotics while awaiting CSF results.
SUBARACHNOID HEMORRHAGE
History of a “thunderclap headache” or “worst headache of life” can be suggestive of subarachnoid hemorrhage. In addition, focal neurologic deficits can be present on examination. A third nerve palsy suggests a possible posterior communicating (PComm) artery aneurysm, whereas a sixth nerve palsy can suggest a posterior fossa lesion or increased intracranial pressure, as can nystagmus or ataxia. Bilateral leg weakness or abulia may signify an anterior communicating (AComm) artery aneurysm; aphasia, hemiparesis, or neglect can suggest a middle cerebral artery (MCA) aneurysm. Patients with these presenting symptoms should undergo immediate noncontrast head CT imaging; if this is negative and subarachnoid hemorrhage is still suspected, lumbar puncture should be performed (checking for the presence of red blood cells or xanthochromia). Note that patients presenting with headache for more than 2 weeks with a negative CT and clear CSF may still have subarachnoid hemorrhage requiring further workup with MRI and vessel imaging with computed tomography angiogram (CTA), magnetic resonance angiogram (MRA), or conventional angiogram.
Only gold members can continue reading. Log In or Register to continue