32 Hemispheric asymmetries
The two cerebral hemispheres are asymmetrical in certain respects. Some of the asymmetries have to do with handedness, language, and complex motor activities; other, more subtle differences come under the general rubric of cognitive style. (Limbic asymmetries are described in Ch. 34.)
Handedness and Language
Language areas
Broca’s area (Figure 32.1)
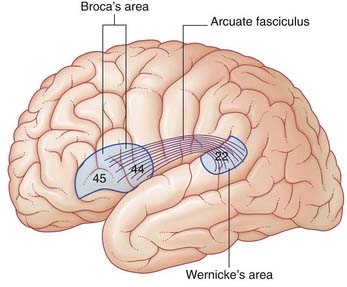
Lesions involving Broca’s area are associated with expressive aphasia (see Clinical Panel 32.1). Some workers believe that expressive aphasia requires that the lesion also includes the lower end of the precentral gyrus.
Clinical Panel 32.1 The aphasias
Motor (anterior) aphasia
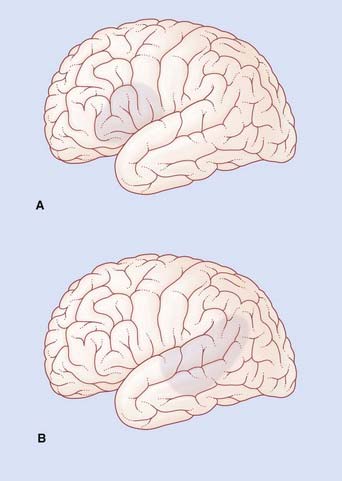
If the lesion involves a substantial amount of the cortical territory of the middle cerebral artery, there will be a motor weakness of the right lower face and right arm. Because the lips and tongue are affected on the right side, the patient will also have dysarthria (difficulty in speech articulation) in the form of slurring of certain syllables. In the example shown in Figure CP 32.1.1A, Broca’s aphasia would be associated with right-sided weakness of the lower face but not of the arm, together with some dysarthria.
Sensory (posterior) aphasia
In the example shown in Figure CP 32.1.1B, Wernicke’s aphasia would be associated with alexia (angular gyrus), ideomotor apraxia (supramarginal gyrus) and probably with a right upper quadrant visual deficit (lower fibers of left optic radiation in the temporal white matter).
Wernicke’s area (Figure 32.1)
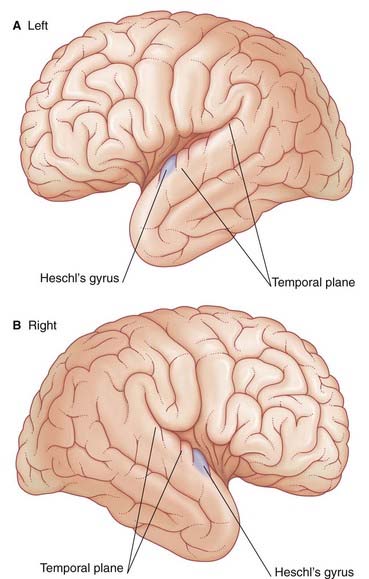
The German neurologist Karl Wernicke made extensive contributions to language processing in the late 19th century. He designated the posterior part of area 22 in the superior temporal gyrus of the left hemisphere as a sensory area concerned with understanding the spoken word. The upper surface of Wernicke’s area is called the temporal plane (Figure 32.2). The volume of cerebral cortex in the temporal plane is larger on the left side in 60% of subjects. The horizontal part of the lateral fissure is longer in consequence – a feature readily identified on MRI scans. Lesions involving Wernicke’s area in adults are associated with receptive aphasia (see Clinical Panel 32.1).
Wernicke’s area is linked to Broca’s area by association fibers of the arcuate fasciculus curving around the posterior end of the lateral fissure within the underlying white matter (Figure 32.1). The two areas are also linked through the insula.
Maldevelopment of the left temporal plane is a significant feature in cases of schizophrenia (Clinical Panel 32.4).
Right hemisphere contribution
During normal conversation there is some increase in blood flow in areas of the right hemisphere matching those of the left. These areas are believed to be concerned with melodic aspects of speech – the cadences, emphases, and nuances, collectively called prosody. Disturbances of the melodic function are called aprosodias (Clinical Panel 32.1).
Angular gyrus
The angular gyrus (area 39) belongs descriptively to the inferior parietal lobule. The left angular gyrus receives a projection from the inferior part of area 19 (the lingual gyrus, shown in Figure 2.6), and itself projects to the temporal plane. It is commonly included as a part of Wernicke’s area.
Listening to spoken words
Figure 32.3 contrasts regional increases in blood flow during PET scanning when a volunteer listens to words (‘active listening’) vs random tone sequences (‘passive listening’). As expected, tone sequences activate the primary auditory cortex (bilaterally). Wernicke’s area (left side) also becomes active, probably in screening out this non-verbal material from further processing. Area 9 in the frontal lobe is thought to be part of a supervisory, vigilance system.
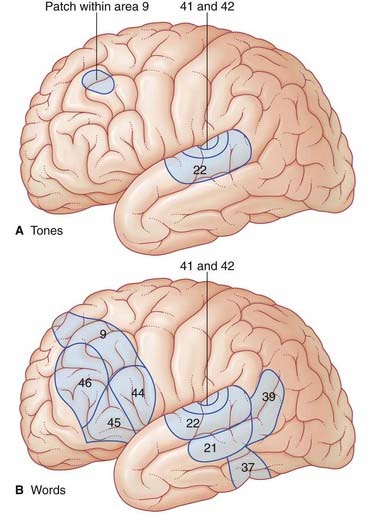
When listening to one’s own voice, the areas of the temporal lobe identified above become active. An important function being served here is meta-analysis (post hoc analysis) of speech, whereby ‘slips of the tongue’ can be identified. Speech meta-analysis is singularly lacking in cases of receptive aphasia (Clinical Panel 32.1).









