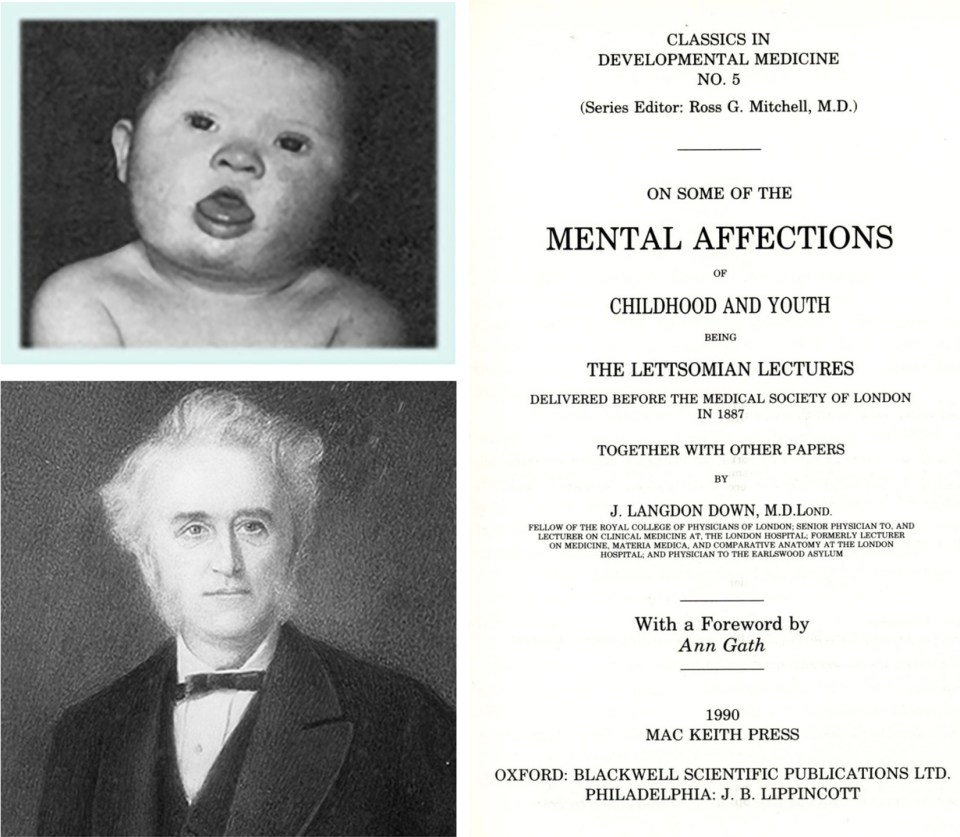
Elizabeth Heada,*; Mark Mapstoneb; Ira T. Lottb,c a Department of Pathology & Laboratory Medicine, University of California, Irvine, CA, United States Introduction to the book that provides a brief history of Down syndrome, provides information on the link between Down syndrome and Alzheimer’s disease, and briefly describes each upcoming chapter. Alzheimer’s disease; Beta-amyloid; Down syndrome; History; Trisomy 21 Our goal for this book is to provide an overview of key topics related to aging and the development of Alzheimer’s disease (AD) in people with Down syndrome (DS). We envision that this book will be useful to students, researchers and physicians, healthcare professionals, and to interested family members. We have assembled leaders in the field to provide chapters in their areas of expertise representing the cutting edge of research both nationally and internationally. In this introduction, we will review some background information that will set the stage for the chapters and provide context. The clinical features of Down syndrome (DS) were initially described by J. Langdon Down in 1866 [1, 2] (Fig. 1) but it was not until 1959 when the most common cause of DS was identified as a chromosome 21 trisomy by Drs. Lejeune, Gautier, and Turpin in 1959 [3] (Fig. 2). An extra copy of chromosome 21 is due to meiotic nondisjunction or the abnormal segregation of the chromosomes during gamete formation (reviewed in Ref. [4]) and accounts for 95% of the people with DS. Interestingly, there are two additional causes of DS that includes partial trisomy 21 (~ 4%) and somatic mosaicism (less than 1%) [4, 5]. Of course what has become known as Down syndrome existed before these seminal descriptions, much less is known about the early history of the condition prior to the 19th century. It is interesting to note that there is evidence of children with DS dating back to the 5–6th century AD based upon a study of the “Saint-Jean-des-Vignes child,” in the painting titled The Adoration of the Christ Child (c. AD 1515) [6, 7] (Fig. 3), which was found in a burial site. Children with DS were have been depicted in several art pieces with a thorough discussion of several paintings described by John M. Starbuck (https://docs.lib.purdue.edu/cgi/viewcontent.cgi?article=1019&context=jca). DS or trisomy 21 is one of the most common causes of intellectual disability and recent national prevalence estimates suggest that 1 in 790 babies are born with DS [8]. This gives us an estimate of approximately 206,366 people with DS in the United States [8], a substantial increase in the population from 1950 of 49,923 people. In Europe, recent estimates suggest that from 2011 to 2015 there were 8031 annual live births of children with DS and a total population of people with DS estimated at 572,000. Of note, selective terminations after prenatal testing have decreased the numbers of children born with DS on average, 54%, leading to an overall 27% reduction in the population [9]. DS is associated with characteristic facial features, deficits in the immune and endocrine systems, and delayed cognitive development (Fig. 4). A full discussion of these conditions, and contribution to aging, are described in Chapters 11 and 13. Improvements in medical care for children and adults with DS, along with more enriched lifestyles, have led to significant extensions in lifespan and enhanced quality of life [10, 11]. As a consequence, up to age 35 years, mortality rates are comparable in adults with DS to individuals with intellectual disability from other causes [12]. Studies in the late 1990s suggested that after age 35, mortality rates doubled every 6.4 years in people with DS as compared to every 9.6 years for people without DS [12]. These statistics are still improving with estimates from 2010 suggesting that 28% of people with DS are living past 40 years of age, as compared with 4% in the 1950s [8]. Indeed, the number of people with DS over the age of 40 years is rapidly rising (Fig. 5). Thus, in the coming decades there will be an increasing need to address age-associated health issues and the development of dementia in this vulnerable population.
Chapter 1: Introduction
b Department of Neurology, University of California, Irvine, CA, United States
c Department of Pediatrics, School of Medicine, University of California, Irvine, Orange, CA, United States
* Corresponding author: heade@uci.edu
Abstract
Keywords
History


Prevalence of DS and phenotype

People with DS are living longer

Related posts:
 Co-occurring medical conditions in aging adults with Down syndrome
Co-occurring medical conditions in aging adults with Down syndrome
 Proteomic and metabolomic biomarkers of Alzheimer’s disease: Opportunities to advance precision medicine and clinical trials
Proteomic and metabolomic biomarkers of Alzheimer’s disease: Opportunities to advance precision medicine and clinical trials
 Fluid biomarkers for Alzheimer’s disease in Down syndrome: Current status and novel trends
Fluid biomarkers for Alzheimer’s disease in Down syndrome: Current status and novel trends
 The contribution of inflammation to Alzheimer’s disease in Down syndrome
The contribution of inflammation to Alzheimer’s disease in Down syndrome
 Magnetic resonance imaging biomarkers for cognitive decline in Down syndrome
Magnetic resonance imaging biomarkers for cognitive decline in Down syndrome
 PET imaging in Down syndrome and Alzheimer’s disease
PET imaging in Down syndrome and Alzheimer’s disease
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Neupsy Key
Fastest Neupsy Insight Engine
