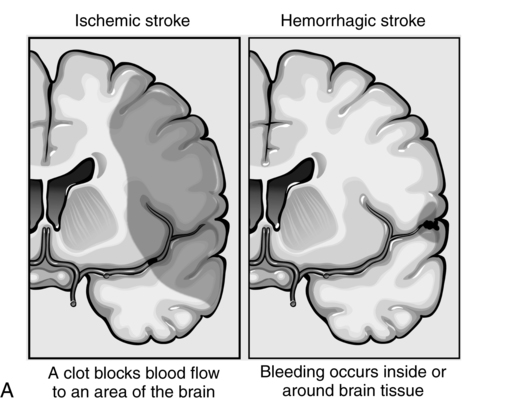
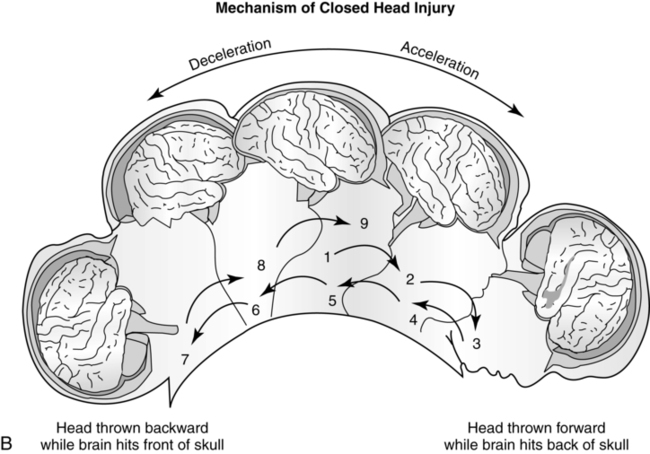
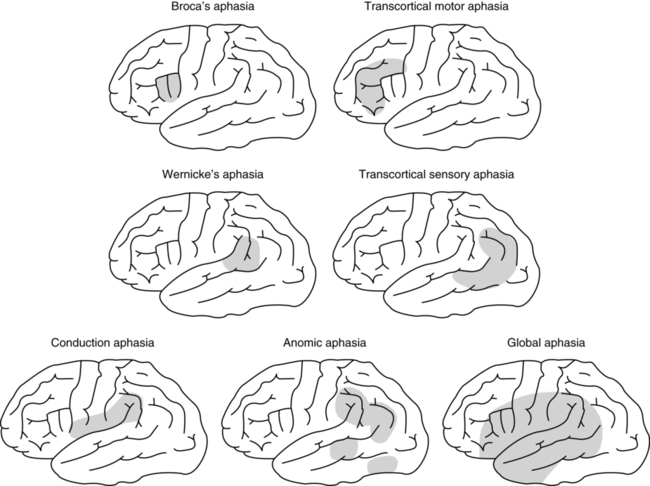
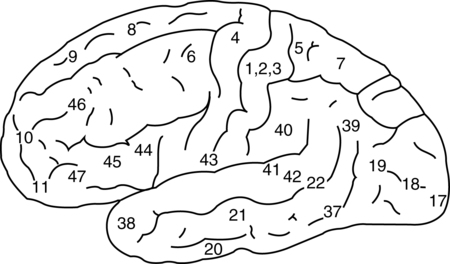
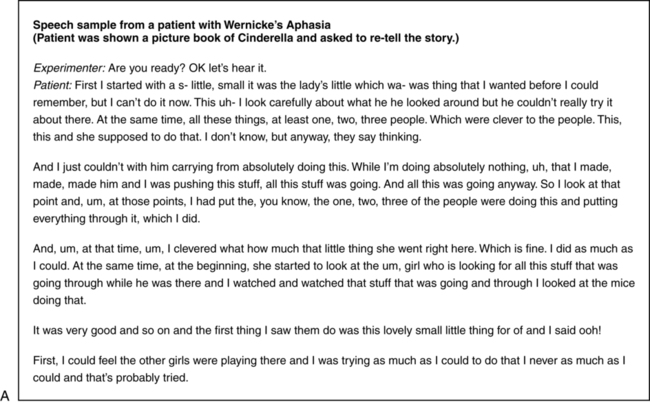
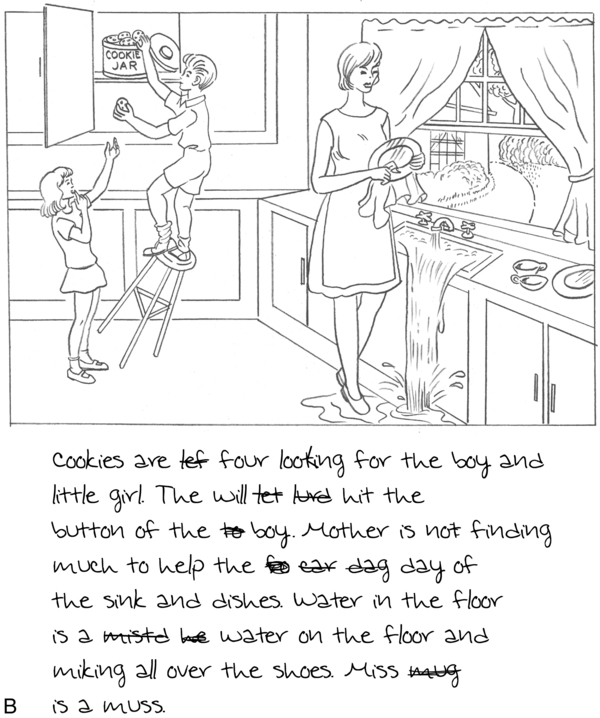
CHAPTER 10 The goal of this chapter is to examine the nature and time-course of language processing in individuals who have survived brain damage. We discuss acquired language disorders and their potential underpinnings from a processing perspective. Our discussion is based upon an examination of the psychological evidence for disordered sentence-level1 language processing in acquired language disorders. Alongside this evidence, we examine specific neural regions that, when damaged, lead to aberrant language processing. Finally, our third principle is that evidence from language disorders arising from localized, acquired neural trauma (specifically stroke) can help illuminate the functional roles of brain regions that are (critically) involved in language processing (Box 10-1). Box 10-1 Focal Versus Diffuse Neural Trauma and Language Disorders From Brain Injury News and Information Blog http://braininjury.blogs.com What is to be gained by such explorations? By understanding the different levels of language processing and the neural and cognitive architectures underlying them, we hope to learn how and when they interact in the unimpaired listener. Such investigations aid us in understanding how language processing is disrupted once brain damage occurs, and may aid in refining neurologically informed models of language processing. A comprehensive and accurate model of the language process could lead to the development of specialized treatment protocols for individuals with language disorders (see Chapter 14). A brief historical review of early research into language processing disorders will help to illustrate how contemporary research in the field has emerged. Prior to the 1800s, there were numerous reports of language disturbances in individuals who had sustained some type of brain injury. However, there was little attempt to correlate particular disorders with specific injuries. Much of what we now know about how the brain processes language first arose during the mid to late 1800s in published case and group study reports of individuals who had acquired language impairments subsequent to a stroke. This language disorder is now referred to as aphasia and is characterized by an impaired ability to produce and/or comprehend language in the spoken, signed or written modalities (see Appendix 10-1 for a more detailed timeline of the field). Aphasia arises secondary to neural trauma (typically stroke) and impedes the proper functioning of brain regions that support language. In most individuals, this involves damage to the left hemisphere of the brain. Aphasia is not the result of deficits in sensory, intellect, or with psychiatric functioning.2 It is also not due to muscle weakness or a general cognitive disorder, though there are those who suggest that cognitive processes such as attention and memory are compromised in aphasia, as well as language (see Chapters 8 and 9). The study of aphasia through history, which can be traced to as early as the Egyptian era (3000 to 2500 bc), has been an interesting, albeit winding road. Often influenced, and usually limited by, erroneous contemporary beliefs ranging from the functional roles of human organs to explanations of human behavior, it is not surprising that we find contradictory hypotheses. Aristotle (c. 360 bc) linked the localization of mental function to the heart, although centuries earlier, ancient Egyptians had already associated language expression with head injuries (Edwin Smith Surgical Papyrus, see Breasted, 1930; Garcia-Albea, 1999). Still others focused on the relationship between language deficits and intelligence or general cognitive function (see Appendix 10-1). In 1861 French neurologist Dr. Paul Broca provided perhaps the most well-known initial description of a language impairment subsequent to focal brain damage (Broca, 1861). In a now famous case, Broca described a patient who had lost the ability to produce speech, with the exception of a single word (“tan”), yet demonstrated spared comprehension. Upon the patient’s death and subsequent autopsy, Broca discovered damage to the left inferior frontal region of this patient’s brain (Figure 10-1, BA 44-45), and he therefore attributed speech output abilities to this circumscribed neural region. In this way, “Broca’s aphasia” came to be known as primarily a speech production disorder following damage to left inferior frontal regions of the brain. Ten years later, German neurologist Dr. Karl Wernicke was also investigating the relationship between localized brain damage and language impairments (Wernicke, 1874). He noted that language deficits could occur following damage to parts of the brain other than the left inferior frontal region, and that symptoms differed depending on the brain regions involved. Specifically, Wernicke posited a link between the left superior temporal gyrus and language comprehension (see Figure 10-1), after observing that patients with damage to this region demonstrated comprehension impairments. From this, “Wernicke’s aphasia” was characterized as a disorder of language comprehension following damage to the left superior temporal gyrus. It was the work of Broca and Wernicke that spurred early investigations of brain injury and its effect on language (among other behaviors). Two important observations should be noted regarding “aphasia” research during this time.3 First, scientists were operating under the assumption that particular language functions (e.g., production, auditory comprehension) were controlled by specific neural regions, and thus assumed that damage to that region resulted in a specific language deficit. While this characterization of brain–behavior relationships is intuitively appealing, later in this chapter we will discuss how a good deal of research has since shown this line of thought to be inadequate. Language is much more complex than a simple “input–output” system. During the early era of aphasia research, the field of aphasiology was descriptive—language disorders were characterized based on direct observable behaviors (i.e., the patient’s overt symptoms). However, several years after Broca and Wernicke described patterns of language impairment in their patients, the Wernicke-Lichtheim model was introduced (Lichtheim, 1885), which marked the first attempt to predict patterns of aphasia following stroke. This model, shown in Box 10-2, anticipated aphasia subtypes, or groups, based on symptoms and site of neural trauma. Symptoms were cast in terms of language activities, like speaking and listening; “lesions” (injury) within the core areas and the connections between them were used to predict patterns of language impairment in aphasia. For example, damage to the motor center would yield a Broca’s type of aphasia, while a lesion to the auditory center would yield a Wernicke’s type of aphasia. A lesion to the auditory-motor pathway would yield a disconnection syndrome, such as conduction aphasia, characterized by the inability to repeat what is heard. Hence, this model ushered in an era of aphasiology that could be characterized as “connectionism.4” During this era, connectionism assumed that higher mental functions were dependent on the connections between different centers in the cortex (Ahlsén, 2006). A more modern proponent of connectionism, Norman Geschwind, advanced the theory that disconnections between neural regions could lead to language disturbances (Geschwind, 1965). Connectionism remained an important concept in aphasiology for many years (and variants of this work remain active topics of research). Box 10-2 Adaptation of the Wernicke-Lechtheim Model of Language Disturbance in Aphasia The contemporary era of aphasia research (and the focus of this chapter) was ushered in by Caramazza and Zurif (1976) and others, who examined the dissociation between different levels of language processing deficits in aphasia (see Accounts of Language Deficits in Aphasia later in this chapter). Indeed, current research aims to uncover the processing deficits in aphasia that may account for observable language deficits. Before we discuss this process-oriented research, we first introduce and briefly describe the major types/syndromes of aphasia, to set the stage for a discussion of processing differences between these syndromes. Broca’s aphasia is typically characterized by halting, nonfluent speech. Grammatical function words (such as “is,” “and,” “the”) and inflections (for tense, agreement, number, gender), are often omitted in language production (spoken or written), with mainly root content words being produced. Someone with Broca’s aphasia may say “boy girl fall” to mean “The boy and the girl are falling” (Figure 10-2, A, B). Language production is therefore described as telegraphic or agrammatic (“without grammar”). In the 1970s, it was discovered that this agrammatic component of Broca’s aphasia also extends to comprehension. The failure to detect comprehension deficits in Broca’s patients was likely due to the fact that comprehension of single words and simple sentences (mostly) appears relatively intact. We now know that language impairment in Broca’s aphasics extends to comprehension of more complex sentence constructions such as noncanonical structures (i.e., passives and object-relatives, see Chapter 6). This impairment for noncanonical sentences was investigated by Caramazza and Zurif (1976), who noted that Broca’s patients demonstrated poor comprehension for sentences containing reversible noun phrases (e.g., “The boy was chased by the girl,” where either of the nouns boy or girl can perform the action chase). This was in stark contrast to the group’s ability to understand noncanonical sentences that did not contain reversible constituents (e.g., in “The ice cream was eaten by the boy,” only the animate noun boy can perform the action eat, thus reducing the likelihood that patients would believe ice cream to be the subject of the sentence). This finding of Broca’s patients’ difficulty in understanding noncanonical sentence structures led to the term “overarching agrammatism,” which refers to the fact that the grammatical constituents of language are not employed in either the production or comprehension of sentences (this will be discussed in more detail shortly). In addition to agrammatism, repetition abilities may also be impaired in this group (Table 10-1). Table 10-1 Types of Aphasia and Associated Symptomotology Broca’s aphasia, and a subtype known as agrammatic aphasia, commonly occur following damage to the left inferior frontal regions (Figure 10-3).5 However, there have been reports of individuals with Broca’s-like behaviors who have sustained damage to other, subcortical, regions (Alexander, Naeser, & Palumbo, 1987; Fridriksson, Bonilha, & Rorden, 2007), and inconsistencies of this sort make it difficult to precisely characterize brain–behavior relationships. In contrast to the halting, agrammatic speech observed in Broca’s or transcortical motor aphasics, a patient with Wernicke’s aphasia has facile language production and speech that contains grammatical structure. In this type of fluent aphasia, the “preserved” speech fluency originally led researchers to regard Wernicke’s aphasia solely as an impairment of comprehension. Research has since shown, however, that language production in this syndrome is also impaired and typically contains many instances of paraphasias, as exemplified in Table 10-2. Table 10-2 Paraphasias in Wernicke’s aphasia may include jargon or neologistic paraphasias (among others), which are utterances that sound like words of the speaker’s language, but are in fact not real words. For instance, a patient with Wernicke’s aphasia may produce a neologism like “glick,” which is not a true word but conforms to phonological rules of the language (Figure 10-4). Neologisms are suggestive of either impaired word finding or semantic processing in Wernicke’s aphasia. As illustrated in Figure 10-3, damage to the posterior temporal regions is most often implicated in this type of aphasia. Conduction aphasia was originally described by Wernicke. It is classically defined as a disorder of impaired repetition of auditory material. More recent research has indicated that word-finding is impaired in the disorder, and that individuals with conduction aphasia often produce phonemic paraphasias in ongoing speech (Baldo, 2008; Fridriksson, 2010). Injury to the supramarginal gyrus (see Figure 10-1, BA 40) and arcuate fasciculus is commonly associated with conduction aphasia (see Figure 10-3). Global aphasia is the most severe of the aphasia types, in which both language comprehension and production are profoundly impacted, rendering the individual severely impaired. Brain lesions typically span across the frontal and temporal lobes. By contrast, anomic aphasia, or “Anomia,” is perhaps the mildest form of the disorder and is characterized by problems recalling words or names.5 Individuals with this impairment frequently use circumlocutions (speaking in a roundabout way) to express words that they cannot recall or produce. Persons with anomic aphasia may not show other obvious signs of impairment and may in fact produce relatively fluent speech. Comprehension may be mildly impacted in this group with repetition most often intact. Lesion localization in this group is the least reliable of all the aphasias. Most often, there is injury affecting temporal and parietal regions (Fridriksson, 2010). Until the 1970s, it was standard practice to use one methodological approach to examine language ability in patients with language disorders. Typically, this approach took the form of an untimed meta-linguistic task. Such a task measures language processing after the event of interest (e.g., after an entire sentence has been heard). These types of tasks are considered “off-line” measures and reflect what listeners ultimately understand a sentence to mean. They allow individuals to consciously reflect on the problem and use all the resources available to them at the time to determine the final meaning of a sentence. Examples from aphasia research include sentence-picture matching, grammaticality judgment, and paraphrasing (e.g., Caramazza & Zurif, 1976; Friedmann, 2006; Linebarger, Schwartz, & Saffran, 1983) (see Chapter 6, Box 6-2, for additional discussion). To understand the complete details of the comprehension process, language scientists require methods that can capture the moment-by-moment unfolding of comprehension. “On-line” tasks do just this, and allow researchers to observe language processing both while it is occurring and without conscious reflection on the part of the participant. With on-line experimental techniques and the right kinds of experimental designs, researchers can examine the individual stages or components of language processing, and in populations with language disorders, investigate which of these stages may be impaired. In keeping with the goals of this chapter, we briefly summarize on-line methodologies that have been (and are currently) used to study auditory sentence comprehension in Table 10-3 (see also Chapter 6, Box 6-1). Table 10-3 Methodologies Commonly Used in the Study of Language Processing in Aphasia In the realm of production, the Tree Pruning Hypothesis is a predominant linguistically-motivated theory of production deficits in Broca’s aphasia. Within this framework, production deficits are ascribed to impairment among Broca’s patients in the ability to represent elements of a linguistic tree. Consider (1) and (2) (from Friedmann, 2006): Here, the verb walk is inflected for tense (e.g., present or past), and must also agree with the person, gender or number of the subject (e.g., the boy/boys). Now consider Figure 10-5, which represents a linguistic tree structure for such a phrase, and note that Agreement (Agr) and Tense (T) are represented by separate nodes (see Chapter 6 for a discussion of tree structure representations; example from Friedmann, 2006; Pollock, 1989; additional reference from Grodzinsky, 2000a). Here, the important element to note is that Tense is represented at a higher node than Agreement. Interestingly, a good number of cross-linguistic studies (many in which tense and agreement are more richly inflected than in English), have demonstrated that individuals with Broca’s aphasia show dissociation in the production of Agreement and Tense. For example, given the following prompt in (3), participants should produce a verb that is inflected for tense and must agree with the subject (past tense, third-person feminine singular, e.g., “jumped”; from Friedmann & Grodzinsky, 1997):
Language processing disorders
Introduction
From Nucleus Medical Media www.nucleusinc.com
A historical perspective
Predicted Deficit
Pathway
Auditory comprehension
Auditory input
→
Auditory center
→
Concept center
Voluntary speech
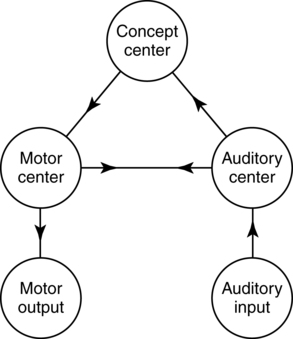
Concept center
→
Motor center
→
Motor output
Repetition
Auditory input
→
Auditory center
→
Motor center
→
Motor output

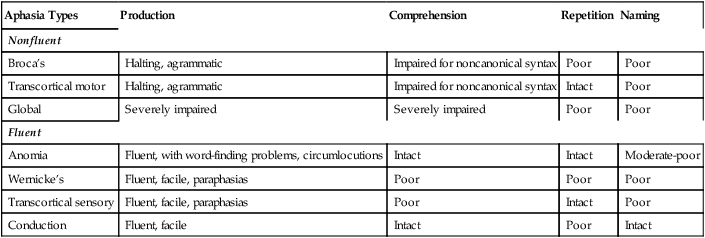
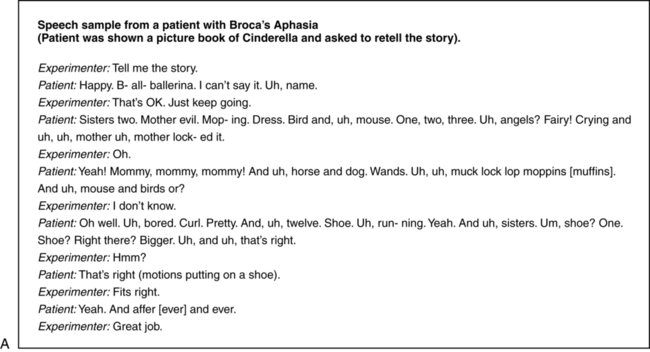
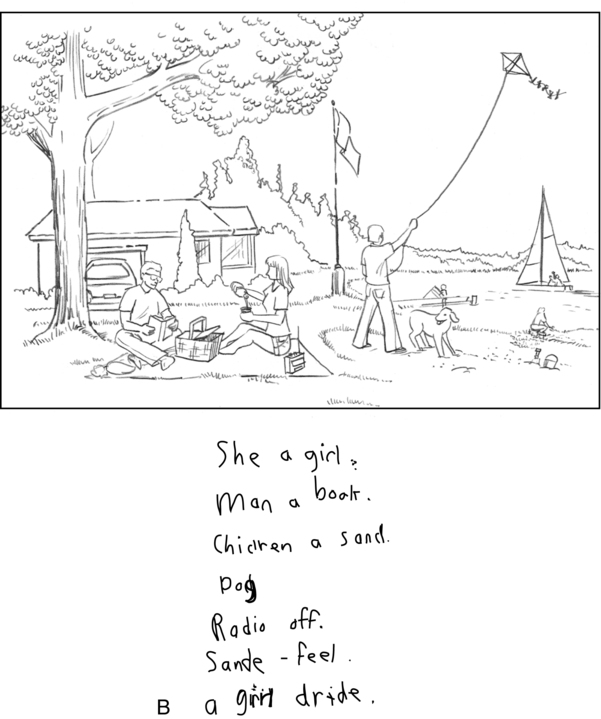
Types of aphasia
Aphasia Types
Production
Comprehension
Repetition
Naming
Nonfluent
Broca’s
Halting, agrammatic
Impaired for noncanonical syntax
Poor
Poor
Transcortical motor
Halting, agrammatic
Impaired for noncanonical syntax
Intact
Poor
Global
Severely impaired
Severely impaired
Poor
Poor
Fluent
Anomia
Fluent, with word-finding problems, circumlocutions
Intact
Intact
Moderate-poor
Wernicke’s
Fluent, facile, paraphasias
Poor
Poor
Poor
Transcortical sensory
Fluent, facile, paraphasias
Poor
Intact
Poor
Conduction
Fluent, facile
Intact
Poor
Intact
Paraphasia Type
Description
Example
Phonemic (Literal)
Substitution of one phoneme for another within a single word
Neologistic (Jargon, Gibberish)
Substitution of word sounds phonetically and semantically unrelated to the target words
/glick/ for /pencil/
Semantic (Verbal)
Substitution of one word for another, but not always semantically related
/flew/ for /soared/

Language processing in aphasia
Methodologies used to study language processing
The study of language processing via off-line methodologies
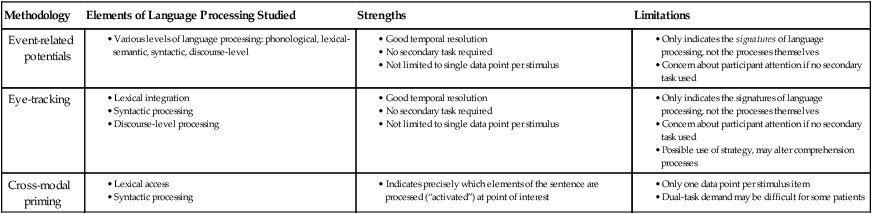
The study of language processing via on-line methodologies
Methodology
Elements of Language Processing Studied
Strengths
Limitations
Event-related potentials
Eye-tracking
Cross-modal priming
Accounts of language deficits in aphasia
Representational accounts of Broca’s aphasia deficits
Production.
Related posts:
 The cognition of language and communication
The effects of aging on language and communication
Treating communication problems in individuals with disordered language
The role of memory in language and communication
Management of acquired language disorders associated with attentional impairment
Language and communication disorders associated with attentional deficits
The cognition of language and communication
The effects of aging on language and communication
Treating communication problems in individuals with disordered language
The role of memory in language and communication
Management of acquired language disorders associated with attentional impairment
Language and communication disorders associated with attentional deficits
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree