4 Late Responses
Nerve conduction studies are most often used to assess distal nerve segments, with routine stimulation seldom done above the elbow or knee. Few studies can be easily performed to assess the more proximal nerve segments (plexus and roots). In the arm, surface stimulation can be performed proximally in the axilla and at Erb’s point, although technical factors limit these studies, especially at Erb’s point. Needle stimulation or high-voltage stimulators, both of which have technical limitations, often are needed to study proximal nerve segments at the root level. In the electromyography (EMG) laboratory, two late responses, the F response and the H reflex, are used routinely to study the more proximal nerve segments. Each has its advantages and limitations (Table 4–1). Although both are usually thought of as assessing only the proximal nerve segments, in reality they travel the entire nerve segment from distal to proximal and back. Thus, they are most useful when routine nerve conduction studies, which assess distal segments, are normal and the late responses are abnormal, a situation that implies a proximal lesion.
Table 4–1 Late Responses: F Response and H Reflex
| F Response | H Reflex | |
|---|---|---|
| Afferent | Motor | Sensory (Ia muscle spindle) |
| Efferent | Motor | Motor |
| Synapse | No | Yes |
| Nerves studied | All | Tibial–soleus (median-FCR, femoral-quads) |
| Stimulation | Supramaximal | Submaximal, long duration pulse (1 ms) |
| Configuration | ||
| Measurements | ||
| Major uses | ||
| Normal values | ||
| Miscellaneous |
CMAP, compound muscle action potential. FCR, flexor carpi radialis.
* Assumes median height, normal conduction velocity and distal latency.
F Response
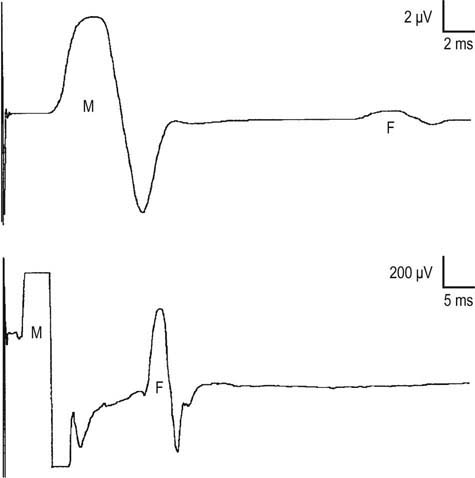
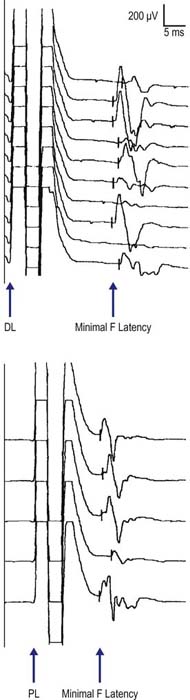
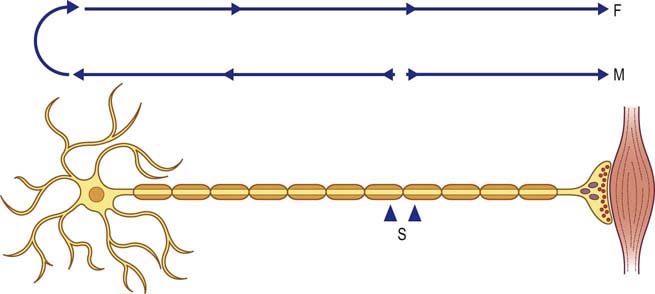
The F response is a late motor response that occurs after the compound muscle action potential (CMAP, also known as the direct motor [M] potential) (Figure 4–1). The F response derives its name from the word “foot” because it was first recorded from the intrinsic foot muscles. In the upper extremity, when the median or ulnar nerves are stimulated at the wrist, the F response usually occurs at a latency of 25 to 32 ms. In the lower extremity, when the peroneal or tibial nerves are stimulated at the ankle, the F response usually occurs at a latency of 45 to 56 ms. If the stimulator is moved proximally, the latency of the CMAP increases as expected, but the latency of the F response actually decreases (Figure 4–2). This is due to the circuitry of the F response, which is initially antidromic toward the spinal cord. Thus, with more proximal stimulation, the action potential has less distance to travel, hence the shorter latency. During a routine motor nerve conduction study, one usually thinks of the action potential as traveling down the nerve across the neuromuscular junction (NMJ) to subsequently depolarize the muscle. When stimulated, however, the nerve conducts well in both directions. The F response is derived by antidromic travel up the nerve to the anterior horn cell, with backfiring of a small population of anterior horn cells, resulting in orthodromic travel back down the nerve past the stimulation site to the muscle (Figure 4–3). The F response is actually a small CMAP, representing 1 to 5% of the muscle fibers. The F response circuitry, both afferent and efferent, is therefore pure motor. There is no synapse, so it is not a true reflex. In conditions that selectively affect the sensory nerves or sensory nerve roots, the F responses are completely normal.
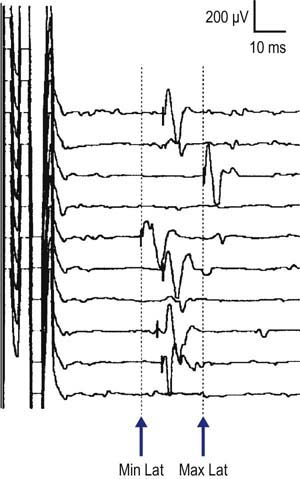
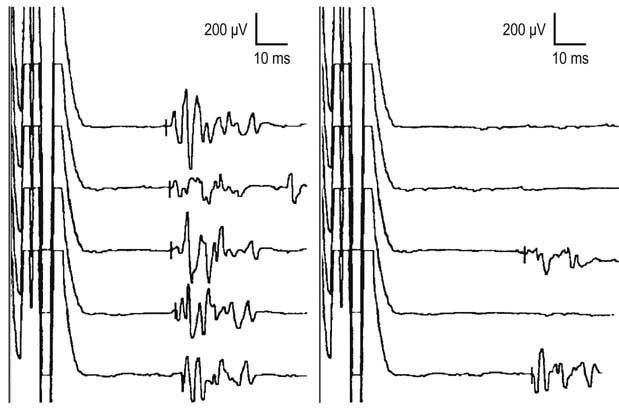
Each F response varies slightly in latency, configuration, and amplitude because a different population of anterior horn cells is activated with each stimulation. Presumably, the shortest latency represents the largest and fastest conducting motor fibers. Several measurements can be made on the F responses, with the most common being the minimal (or fastest) F response latency (Figure 4–4). F wave persistence is a measure of the number of F waves obtained per the number of stimulations. Normal F wave persistence is between 80 and 100%, and always above 50% with the exception of the peroneal F responses (see below). F wave chronodispersion is a measure of the difference between the minimal (fastest) and maximal (slowest) F response latency. Normal chronodispersion is up to 4 ms in the upper extremities and up to 6 ms in the lower extremities. F responses can be obtained from any motor nerve. The only notable exception to this is the peroneal nerve, wherein F responses may be difficult to elicit even in normal subjects. Note also that F responses may be absent or impersistent in all nerves in sleeping or sedated patients. In these situations, absent or impersistent F responses are not necessarily a sign of pathology. F responses are best obtained with distal stimulation. With proximal stimulation, they often are superimposed on the terminal CMAP and may be more difficult to identify.
F Response Procedure
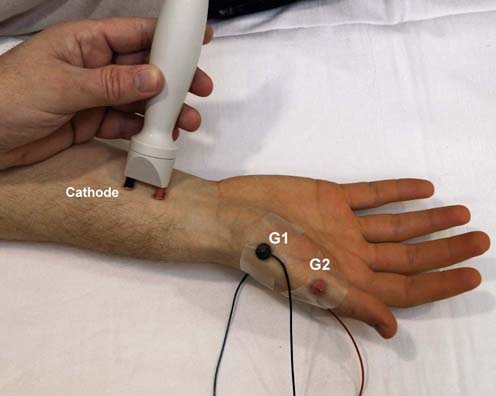
To obtain an F response, the setup is essentially the same as that for a routine motor conduction study using distal stimulation. Several adjustments must be made to the EMG machine to record F responses, however. The gain should be increased to 200 µV (because the amplitude of the F response is quite low), and the sweep speed should be increased to 5 or 10 ms, depending on the length of the nerve being studied. Supramaximal stimulation must always be used, and the stimulator should be turned around so that the cathode is more proximal (Figure 4–5). Although F responses typically can be obtained with the stimulator in the standard position (cathode distal), there is the theoretical possibility of anodal block (wherein the nerve hyperpolarizes under the anode, blocking antidromic travel of the action potential from the depolarization site under the cathode). One should stimulate at a rate no faster than once every two seconds (0.5 Hz). This is done in order to avoid the effects of the previous stimulus on a subsequent response. In addition, stimulating at this rate is much more comfortable for the patient and avoids the “temporal summation of pain” that occurs when the stimulation frequency is too fast (i.e., the patient is stimulated again before recovering from the discomfort of the previous one).
Because each F response varies in latency and amplitude, it is important to obtain at least ten F responses, preferably on a rastered trace. Indeed, the normal values of F waves are based on doing at least ten stimulations. If one is unable to obtain an F response, first ensure that the nerve has been stimulated supramaximally. Second, the Jendrassik (reinforcement) maneuver can be of help in “priming” the anterior horn cells. The patient can be asked to make a fist with the contralateral hand or clench the teeth prior to each stimulation. This maneuver often will elicit an F response where one was not present at rest. It should be noted that one should not do the Jendrassik maneuver unless the F responses are difficult to elicit. Paradoxically, performing a Jendrassik maneuver when not necessary can actually decrease the likelihood of obtaining F responses.*
Of the various F response measurements (minimal latency, chronodispersion [maximal minus minimal F response latency], and F wave persistence [Figure 4–6]), the minimal F wave latency is the most reliable and useful measurement, although occasionally side-to-side differences in F wave persistence and chronodispersion help in identifying an abnormality. Unfortunately, because F responses are quite small, there is often some inherent error in placing the latency markers. It is best to place the latency marker on the F response at the point where it departs from the baseline, with either a positive or negative deflection. In addition, superimposing the rastered traces once all the responses are obtained is often helpful in determining the minimal latency.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


