Chapter 20 Lumbar Plexus and Sacral Plexus
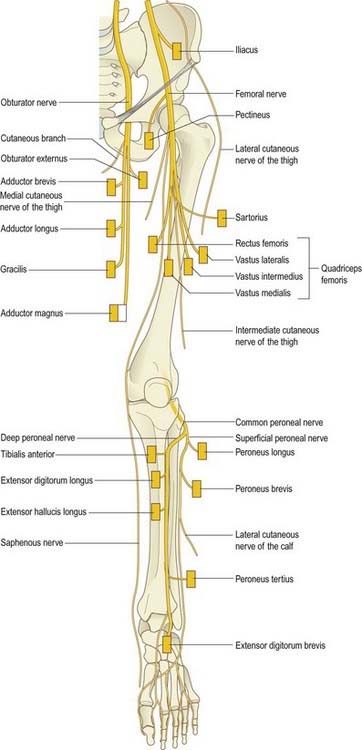
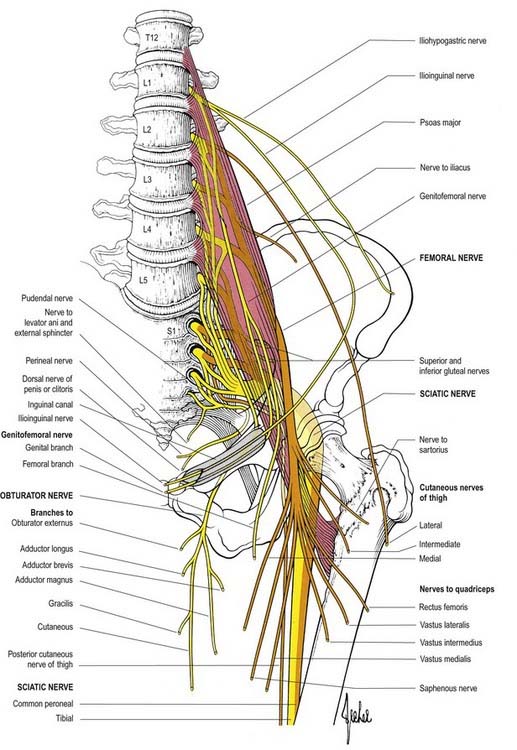
Overview of the Principal Nerves of the Lower Limb (Figs 20.1, 20.2)
Femoral Nerve (L2–4)

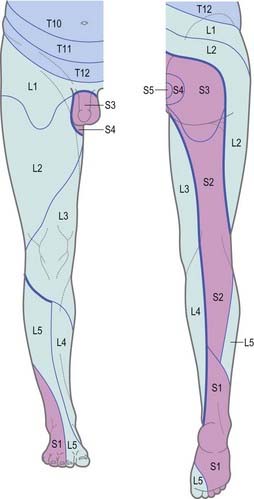
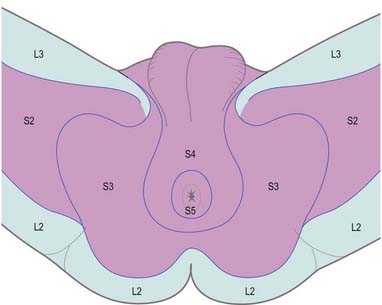
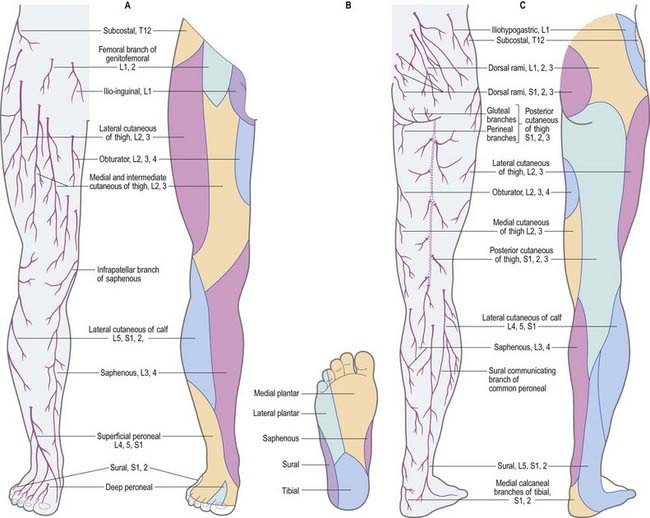
Dermatomes
Our knowledge of the extent of individual dermatomes, especially in the limbs, is based largely on clinical evidence. The dermatomes of the lower limb arise from spinal nerves T12 to S3 (Figs 20.3–20.5).
Myotomes
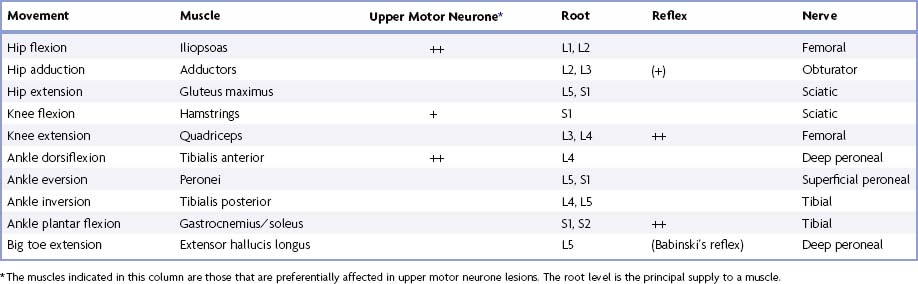
Tables 20.1 to 20.4 summarize the predominant segmental origin of the nerve supply for each of the lower limb muscles and for movements that take place at the joints of the lower limb. Damage to these segments or to their motor roots results in maximal paralysis.
Table 20.1 Movements, muscles and segmental innervation in the lower limb
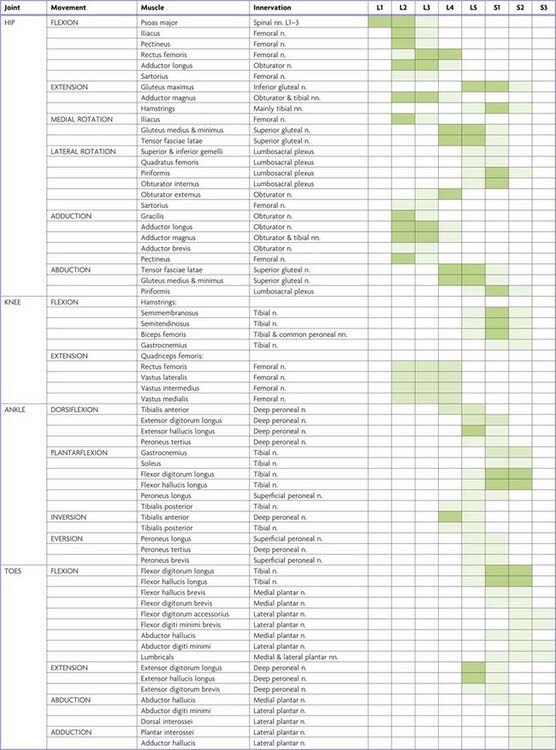
Table 20.2 Segmental innervation of muscles of the lower limb
| L1 | Psoas major, psoas minor |
| L2 | Psoas major, iliacus, sartorius, gracilis, pectineus, adductor longus, adductor brevis |
| L3 | Quadriceps, adductors (magnus, longus, brevis) |
| L4 | Quadriceps, tensor fasciae latae, adductor magnus, obturator externus, tibialis anterior, tibialis posterior |
| L5 | Gluteus medius, gluteus minimus, obturator internus, semimembranosus, semitendinosus, extensor hallucis longus, extensor digitorum longus, peroneus tertius, popliteus |
| S1 | Gluteus maximus, obturator internus, piriformis, biceps femoris, semitendinosus, popliteus, gastrocnemius, soleus, peronei (longus and brevis), extensor digitorum brevis |
| S2 | Piriformis, biceps femoris, gastrocnemius, soleus, flexor digitorum longus, flexor hallucis longus, some intrinsic foot muscles |
| S3 | Some intrinsic foot muscles (except abductor hallucis, flexor hallucis brevis, flexor digitorum brevis, extensor digitorum brevis) |
Table 20.3 Segmental innervation of joint movements of the lower limb
| Hip | Flexors, adductors, medial rotators | L1–3 |
| Extensors, abductors, lateral rotators | L5, S1 | |
| Knee | Extensors | L3, L4 |
| Flexors | L5, S1 | |
| Ankle | Dorsiflexors | L4, L5 |
| Plantar flexors | S1, S2 | |
| Foot | Inverters | L4, L5 |
| Everters | L5, S1 | |
| Intrinsic muscles | S2, S3 |
Lumbar Plexus
The posterior abdominal wall contains the origin of the lumbar plexus (Fig. 20.6) and numerous autonomic plexuses and ganglia that lie close to the abdominal aorta and its branches.
Lumbar ventral rami increase in size from first to last and are joined, near their origins, by grey rami communicantes from the four lumbar sympathetic ganglia. These rami, long and slender, accompany the lumbar arteries around the sides of the vertebral bodies, behind psoas major. Their arrangement is irregular: one ganglion may give rami to two lumbar nerves, or one lumbar nerve may receive rami from two ganglia. Rami often leave the sympathetic trunk between ganglia. The first, second and sometimes third lumbar ventral rami are each connected with the lumbar sympathetic trunk by a white ramus communicans. The lumbar ventral rami descend laterally into psoas major. The first three and most of the fourth form the lumbar plexus; the smaller moiety of the fourth joins the fifth as a lumbosacral trunk, which joins the sacral plexus. The fourth is often termed the nervus furcalis, being divided between the two plexuses; however, the third is occasionally the nervus furcalis. Alternatively, both the third and fourth may be furcal nerves, in which case the plexus is termed ‘prefixed.’ More frequently, the fifth nerve is furcal, and the plexus is then termed ‘postfixed.’ These variations modify the sacral plexus.
The branches of the lumbar plexus are as follows:
| Muscular | T12, L1–4 |
| Iliohypogastric | L1 |
| Ilioinguinal | L1 |
| Genitofemoral | L1, L2 |
| Lateral femoral cutaneous | L2, L3 |
| Femoral | L2–4 dorsal divisions |
| Obturator | L2–4 ventral divisions |
| Accessory obturator | L2, L3 |
Division of constituent ventral rami into ventral and dorsal branches is not as clear in the lumbar and lumbosacral plexuses as it is in the brachial plexus. Anatomically, the obturator and tibial nerves (via the sciatic) arise from ventral divisions, and the femoral and peroneal nerves (via the sciatic) arise from dorsal divisions. Lateral branches of the twelfth thoracic and first lumbar ventral rami are drawn into the gluteal skin, but otherwise, these nerves are typical. The second lumbar ramus is difficult to interpret. It not only contributes substantially to the femoral and obturator nerves but also has an anterior terminal branch (genital branch of the genitofemoral) and a lateral cutaneous branch (lateral femoral cutaneous nerve and femoral branch of the genitofemoral). Anterior terminal branches of the third to fifth lumbar and first sacral rami are suppressed, but the corresponding parts of the second and third sacral rami supply the skin of the perineum.
Muscular Branches
Small branches are derived from all five lumbar roots.
Iliohypogastric Nerve
Distribution
The iliohypogastric nerve originates from the L1 ventral ramus. It emerges from the upper lateral border of psoas major and crosses obliquely behind the lower renal pole and in front of quadratus lumborum. Above the iliac crest it enters the posterior part of transversus abdominis. Between transversus abdominis and internal oblique, it divides into lateral and anterior cutaneous branches and also supplies both muscles. The lateral cutaneous branch runs through the internal and external oblique above the iliac crest, a little behind the iliac branch of the twelfth thoracic nerve, and is distributed to the posterolateral gluteal skin. The anterior cutaneous branch runs between and supplies the internal oblique and transversus abdominis. It runs through the internal oblique approximately 2 cm medial to the anterior superior iliac spine and through the external oblique aponeurosis approximately 3 cm above the superficial inguinal ring; it is then distributed to the suprapubic skin. The iliohypogastric nerve connects with the subcostal and ilioinguinal nerves (see Fig. 19.3). It is occasionally injured during an oblique surgical approach to the appendix. However, because the suprapubic skin is innervated from several sources, there is rarely any detectable sensory loss. Division of the iliohypogastric nerve above the anterior superior iliac spine may weaken the posterior wall of the inguinal canal and predispose to the formation of a direct hernia.
Lateral Femoral Cutaneous Nerve of the Thigh
The lateral (femoral) cutaneous nerve of the thigh arises from the dorsal branches of the second and third lumbar ventral rami and emerges from the lateral border of psoas major, crossing the iliacus obliquely toward the anterior superior iliac spine. It supplies the parietal peritoneum in the iliac fossa. The right nerve passes posterolateral to the caecum, separated from it by the fascia iliaca and peritoneum; the left passes behind the lower part of the descending colon. Both pass behind or through the inguinal ligament, variably medial to the anterior superior iliac spine (commonly about 1 cm) and anterior to or through sartorius into the thigh, where they divide into anterior and posterior branches. The anterior branch becomes superficial approximately 10 cm distal to the anterior superior iliac spine and supplies the skin of the anterior and lateral thigh as far as the knee. It connects terminally with the cutaneous branches of the anterior division of the femoral nerve and the infrapatellar branch of the saphenous nerve, forming the peripatellar plexus. The posterior branch pierces the fascia lata higher than the anterior, and it divides to supply the skin on the lateral surface from the greater trochanter to about mid thigh. It may also supply the gluteal skin (see Case 2).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


