12 Maxillary and Ethmoid Sinuses in Skull Base Surgery
Nobuyoshi Otori, Kiyoshi Yanagi, and Hiroshi Moriyama
 Introduction
Introduction
Endoscopic ethmoidal surgery and maxillary surgery are the first step in endoscopic skull base surgery. Ethmoid air cells are removed to make the ethmoid sinus unique cavity. The ostium of the maxillary sinus is opened to make a large communication to nasal cavity. These operations make it easy to perform subsequent skull base surgery.
This chapter describes the anatomy and basic techniques of endoscopic sinus surgery for the ethmoid sinus and the maxillary sinus.
 Anatomy of Ethmoid Sinus and Maxillary Sinus
Anatomy of Ethmoid Sinus and Maxillary Sinus
The maxillary sinus is large unique cavity, but the ethmoid sinus is divided into 10 to 20 small air cells. Therefore, when the surgeon approaches the skull base via the ethmoid sinus, it is necessary to make the ethmoid sinus a unique cavity by removing a partition of these small air cells.1–3
The airflow tract of the frontal sinus, anterior ethmoid sinus, and maxillary sinus are called the ostiomeatal complex (OMC) or the ostiomeatal unit (OMU) (Fig. 12.1). It includes the ostium of the frontal sinus, the nasofrontal duct, the ostium of the maxillary sinus, the ethmoidal infundibulum, the semilunar hiatus, and the middle meatus.4
The lamina papyracea is perpendicular in the front, but inclines inward in the rear.4 In addition, the front of the lamina cribrosa is more remarkable than the rear.
The anterior ethmoid sinus is composed of the uncinate process (basal lamella I) and the bulla ethmoidalis (basal lamella II). There is a ground lamella (basal lamella III, basal lamellae of middle turbinate) behind the anterior ethmoid sinus.3 The rear of the ground lamella is a posterior ethmoid sinus. When the surgery advances into the posterior ethmoid sinus, a skull base appears above. The next lamella is a superior turbinate (basal lamellae IV). The rear of the lamella is an anterior wall of the sphenoid sinus (Fig. 12.2).
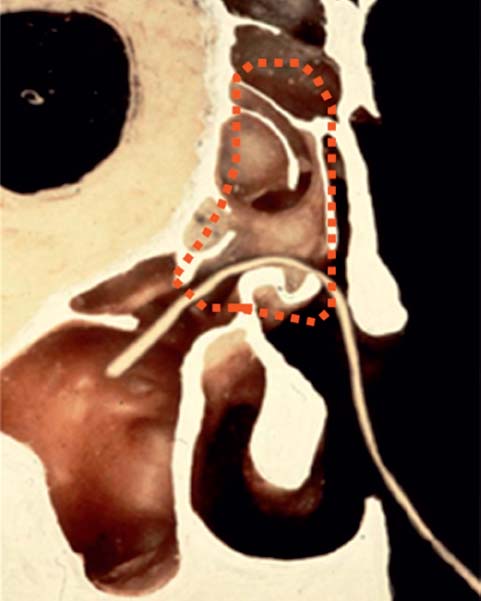
Fig. 12.1 The ostiomeatal complex.
There is sphenopalatine foramen at the end of the ground lamella, and the sphenopalatine artery flows into a nasal cavity from there. In addition, the anterior ethmoidal artery is at the front edge of the ground lamella.
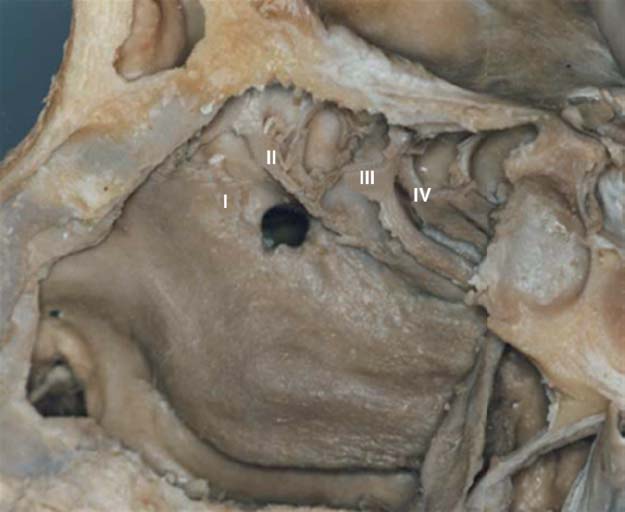
Fig. 12.2 Basal lamellae I to IV on the lateral wall of the nasal cavity.
When the posterior ethmoid sinus grows toward the upper part of the sphenoid sinus, an Onodi cell is formed. In this case the optic canal contacts a rear wall of the posterior ethmoid sinus3,4 (Fig. 12.3).
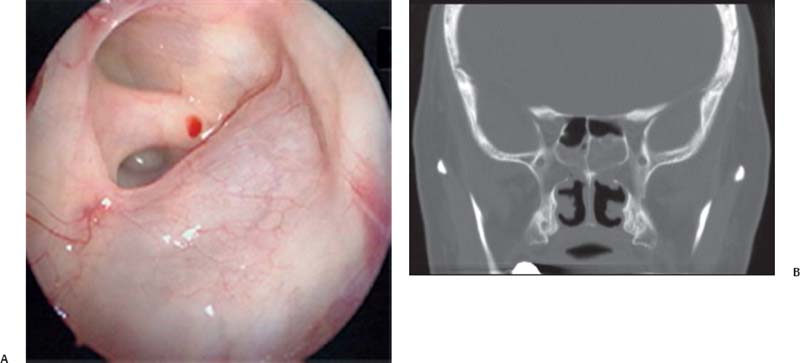
Fig. 12.3 Endoscopic view (A) and computed tomography (CT) scan (B) of the optic canal in the Onodi cell.
 Equipment and Forceps Used for Ethmoid and Maxillary Surgery
Equipment and Forceps Used for Ethmoid and Maxillary Surgery
Ethmoidal and maxillary surgery cannot be performed properly using only conventional forceps.5–7 In addition to Grunwald forceps, a thin forceps, curved forceps, and a microdebrider are also prepared. These instruments facilitate the treatment of lesions of various sites and enable safe and accurate surgery. Curved and flexible aspiration tubes are prepared in addition to the conventional ones. Rigid endoscopes, 0 and 70 degrees with a diameter of 4 mm, are chiefly used, and endoscopes of 30 and 45 degrees are occasionally used.
The selection of forceps is important not only for a safe and accurate operation but also for obtaining good results postoperatively. The through-cutting forceps are used primarily (Fig. 12.4). They are preferred for effective preservation of mucosa and for prevention of injury. Morphologically, the orbit and brain are separated from the paranasal sinuses with a paper-thin bone wall, and periodically part of these bony separations will have dehiscence (Fig. 12.5). Accordingly, pulling the mucosa, lamella, and the bone plate with cuptype forceps is extremely dangerous. Through-cutting forceps are used for safe manipulation in opening the maxillary sinus orifice and for removal of the mucosa and lamella of the ethmoid sinus.
 Surgical Techniques5,6
Surgical Techniques5,6
Understanding the location and variations of the middle turbinate is important, because it serves as an anatomic landmark during the operation. Once the middle turbinate is confirmed, it is pressed medially to widen the middle nasal meatus, and the anterior/posterior ethmoid sinuses are opened by approaching from the middle nasal meatus. In patients with an aerated middle turbinate concha bullosa, the outer wall of the middle turbinate is removed, and then the air cells of the middle turbinate are opened.

Fig. 12.4 Through-cutting forceps.
Related posts:
 External Versus Endoscopic Approaches for Skull Base Malignancies
External Versus Endoscopic Approaches for Skull Base Malignancies
 Transmaxillary Endoscopic Approach to Contralateral Parasellar Lesions
Transmaxillary Endoscopic Approach to Contralateral Parasellar Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


