Meckel Cave Lesion
Anne G. Osborn, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Schwannoma, Trigeminal, Intracranial
Meningioma
Metastasis, Skull Base
Less Common
Metastasis, CSF/Meningeal
Metastasis, Perineural CNV3
Meningitis
Neurosarcoid
Neurofibroma
Pseudotumor, Intracranial
Pituitary Macroadenoma
Rare but Important
Metastasis, Perineural CNV2
Trigeminal Herpetic Neuritis
Lipoma
Epidermoid Cyst
Dermoid Cyst
Neurocysticercosis
Chronic Thrombosis, Dural Sinus
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Normal Meckel cave (MC)
Anatomy
CSF-filled, dura-arachnoid lined invagination into cavernous sinus (CS)
Contains CN5 fascicles, semilunar ganglion
Communicates directly, freely with prepontine/cerebellopontine cisterns
Normal imaging
Ovoid, smooth CSF-filled cisterns on axial, coronal scans resemble “open eyes”
Bilaterally symmetric hypointensity on T1WI
Bilaterally symmetric hyperintensity on T2WI
Abnormal Meckel cave
“Winking” Meckel cave sign
One MC filled with soft tissue, not CSF
One MC therefore NOT = CSF density/intensity
Asymmetric appearance = “Winking” Meckel cave (one “eye” appears closed)
Look for CN5 motor denervation secondary to MC mass
May be only sign of subtle lesion
Acute → hyperintensity, enhancement of muscles of mastication
Chronic → atrophy, fatty infiltration of muscles of mastication
Helpful Clues for Common Diagnoses
Schwannoma, Trigeminal, Intracranial
Variable configuration
“Dumbbell” tumor with CPA component, constriction of tumor at entrance to Meckel cave, Meckel cave mass
May involve MC only
± Extracranial extension along V1, V2, &/or V3
Unilateral unless NF2
Hyperintense on T2WI, strong enhancement on T1 C+
May result in atrophy of muscles of mastication
Meningioma
Uni- > bilateral involvement
Dural thickening along cavernous sinus, tentorium (dural “tail sign”)
± Ipsilateral denervation, atrophy of muscles of mastication
Metastasis, Skull Base
Metastases to Meckel cave can be hematogenous, direct geographic extension, perineural, or CSF spread
Hematogenous spread to central skull base (BOS) with secondary involvement of cavernous sinus
Direct extension from extracranial primary (e.g., nasopharyngeal squamous cell carcinoma) into central BOS
Uni- > bilateral involvement
Sagittal T1WI helpful
Look for replacement of normal fatty clival marrow ± cortical destruction
Helpful Clues for Less Common Diagnoses
Metastasis, CSF/Meningeal
Pia-arachnoid tumor spread may extend into MCs
± Enhancement along cisternal CN5
Metastasis, Perineural CNV3
Retrograde tumor spread along mandibular nerve
Look for mass in retromolar trigone, masticator space
Adenoid cystic carcinoma, squamous cell carcinoma most common
CNV3 appears thick, enhancing ± erosion of foramen ovale
Meningitis
Any etiology (e.g., pyogenic, TB)
Dura-arachnoid disease can extend into MC
Look for basal cistern enhancement
Neurosarcoid
Pituitary gland, infundibular stalk, dural masses common
Can be uni- or bilateral
Neurofibroma
Orbit/scalp/lid plexiform in NF1
May extend posteriorly through SOF, infiltrate V1 branches → MC
Pseudotumor, Intracranial
Typically originates in/around orbit
Extends through SOF into CS, MC
Variable dura-arachnoid thickening, enhancement
Idiopathic invasive subtype
May erode bone, mimic aggressive infection, neoplasm
Pituitary Macroadenoma
Can extend into one or both CSs, MCs
Pituitary gland generally cannot be distinguished from mass
Gland IS mass
Aggressive invasive type may destroy central skull base, clivus
Pituitary adenoma > > > > carcinoma
Can mimic malignant disease, so do endocrine workup
Helpful Clues for Rare Diagnoses
Metastasis, Perineural CNV2
Often skin carcinomas (basal, squamous cell)
Infiltrates along inferior orbital canal
May enlarge/erode foramen rotundum
Thickened, enhancing maxillary nerve
Trigeminal Herpetic Neuritis
Herpes zoster oticus > trigeminal neuritis
Edematous, enhancing CN5
Ophthalmic division most commonly involved
Lipoma
MC is rare site
Uni- > bilateral
Epidermoid Cyst
May originate in MC or as extension from CPA epidermoid
Does not suppress on FLAIR; restricts on DWI
Dermoid Cyst
Looks like fat in MC, not CSF
May occur with or without rupture, CSF fatty droplets
Neurocysticercosis
Cysts in basal cisterns may extend into one or both MCs
Chronic Thrombosis, Dural Sinus
Chronically occluded dural sinus(es)
Dural thickening, enhancement secondary to collateral venous drainage
May involve one or both MCs
Image Gallery
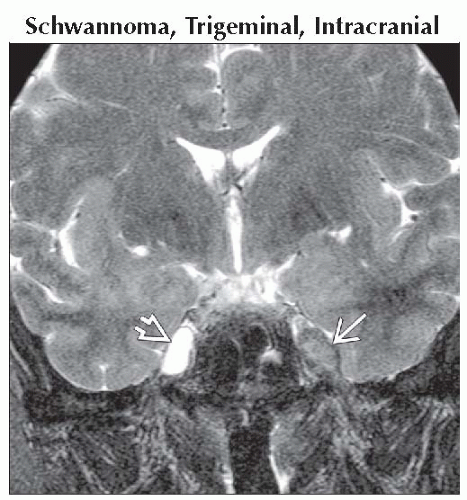 Coronal T2WI MR shows a classic “winking Meckel cave sign”. The normal (right) Meckel cave is CSF-filled, hyperintense
 . The left side is filled with a mass that is hypointense and expands the Meckel cave . The left side is filled with a mass that is hypointense and expands the Meckel cave  . .Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|