12 Motor Control Neuro-Developmental Treatment practice currently draws heavily on elements of dynamic systems (DS) and neuronal group selection (NGS) theories to explain the nature of typical movement, how posture and movement are organized, and how posture and movement change due to impairments in various body systems. This chapter defines motor control and focuses on theories which emphasize the dynamic interplay between brain, body, and environmental context which are fundamental principles of NDT. Learning Objectives Upon completing this chapter the reader will be able to do the following: • Link the importance of NDT assumptions to motor control. • Describe the changes in motor control theories, including reflex/hierarchical theory, motor programs, central pattern generators, dynamic systems theory, and neuronal group selection theory, and relate the tenets of these theories to NDT practice. • Define the tenets of the theory of neural group selection, including developmental selection, primary repertoires, secondary repertoires, and global maps. • Apply tenets of neuronal group selection to the NDT practice model focusing on concurrent changes in the brain and body systems, experience, and context. • Explain the principles of dynamic systems theory, including coordinative structures, self-organization, rate-limiting factors, and state transitions. • Apply dynamic systems theory to NDT practice, particularly focusing on the importance of body systems and environmental contexts when developing intervention strategies. This chapter defines motor control (MC) as an explanation of how the central nervous system (CNS), environment, and body systems interact and organize individual joints and muscles to produce coordinated functional movement. The theories of MC are drawn from various fields of study, each one trying to understand the nature of movement. Theories have changed based on observations of typical and atypical motor behavior and the scientific study of neuronal mechanisms, muscle physiology, cognition and perception, motivation, and purpose—all variables that contribute to initiation and execution of movement. For our purposes a definition of MC must also include how an understanding guides clinical practice. In the late 1930s and ’40s, as the Bobaths sought to explain their clinical observations, like everyone else, they relied on models of MC accepted at that time. They cited reflex/hierarchical theories (R/HTs) based on work from Jackson, Magnus, and Sherrington that linked the control of movement to specific structural levels in the brain.1 These theories assumed that the structures of the brain were organized and developed in a hierarchy and that there was a fixed relationship between function and structure. Each successively higher level of brain structures provided more precise movement integration. Therefore, as these structures developed, function changed accordingly. The lowest level of fundamental movement patterns were sensory-elicited reflexes, which were then integrated into the automatic postural reflex mechanism as the higher brain levels developed. These automatic movements, including righting and equilibrium reactions, were considered to be the basis for skilled voluntary movements. These predictable, reflexive movements were continually modified and refined at each neural level until the final outcome was a rich array of adaptable combinations of automatic postural reactions that supported discrete voluntary movements. It stood to reason, then, that a lesion in the higher neural centers permitted expression of normally suppressed patterns of movement, which would dominate the person’s posture and movement. The R/HTs helped to explain the stereotypic movements and postures seen in persons with neuropathology. These were acceptable neural control models until the late 1960s and, although they did offer explanations for predictable movement seen in cerebral palsy (CP) and stroke, their limitation was that they did not account for context-based movement variability, individuality, novelty, and context-based behaviors. A critical shift in thinking came about in the 1960s and ’70s, as investigators theorized that motor programs stored in the brain, rather than reflexes, were the substrate for motor behavior.2,3 Keele proposed the existence of a set of commands in the CNS that he called motor programs, which were assembled and initiated without sensory input and performed in the absence of peripheral feedback. These motor programs, later called generalized motor programs (GMPs) contain the abstract representation of movement, including the commands for movement, codes of action, and general features of movement sequences as well as the recruitment of appropriate agonists and synergists with adjustment of antagonists.4 For example, there could be basic motor plans for reaching and grasping and rhythmic movements for walking or speaking that are assembled prior to the need to move. Simple sequences could then be linked together to produce complex actions, such as walking down a slope or up a flight of stairs, writing a thesis, reciting poetry, or singing. The richness of the GMPs developed from both experience and learning. As this theory evolved, GMP theory (GMPT) recognized that movement has both variant and invariant features in which variant features could be modified, whereas the invariant features were difficult to change. This was the explanation for changes that were seen following neural insult, as well as the explanation for lack of change. GMPs acknowledged that skilled movement required interactions of both central and peripheral mechanisms.5 GMPT supported the idea that, once learned, an individual’s movements and postures are more or less “automatic” and do not require attention for the individual to perform them effectively and efficiently. These programmed movements acted as the supporting system for the intentional elements of a particular self-initiated movement, much like the postural reflex mechanism was seen as the support system in R/HTs. The emergence of the idea that motor programs were the basic unit of MC renewed the interest in the concept of central pattern generators (CPGs). Investigators became interested in neural networks in the spinal cord capable of producing rhythmic movement even when isolated from the brain and sensory systems. CPGs have been established as the basis for specific rhythmic movements in invertebrates, fish, and cats.6,7 There was increasing evidence that specialized neural circuits do exist in the brain stem of vertebrates for breathing, chewing, and swallowing, and in the spinal cord for locomotive functions.8,9 However, evidence of the existence of CPGs in humans remains indirect.10 The fact that rhythmic movements can be obtained in the absence of supraspinal and sensory inputs should not be interpreted as meaning that these inputs are not important in pattern generation in persons with intact neural systems, but suggests that if rhythmic movements for walking can be elicited in persons with neural impairment, then perhaps this can be a strategy for the development of more adaptive motor behaviors. Partial body-weight-bearing (PBWB) gait training is one intervention that gains support from CPGs. It is a method currently used in conjunction with Neuro-Developmental Treatment (NDT) intervention to train or retrain walking in persons with neuropathology. This intervention uses a support harness to provide alignment, reduce the need for independent balance, and remove the fear of falling. Unweighting the body, particularly when combined with treadmill walking, changes the environmental constraints and makes stepping easier and more rhythmic (Fig. 12.1). Fig. 12.1 Partial body-weight-bearing on a treadmill reduces constraints of balance, and alignment makes stepping easier and more rhythmical. Many researchers and clinicians use GMP and, in particular, CPG theory, to explain improved rhythm between stance and swing in walking patterns in adults with spinal cord injuries and stroke and in children with CP when body weight is partially supported and stepping is encouraged on a treadmill.11,12,13,14 The rhythmical components of reciprocal stepping on a treadmill may be organized by networks of neurons in the spinal cord; however, afferent somatosensory inputs have been shown to be powerful cues that bring about stance-to-swing-phase transitions and promote neuroplasticity in persons with impairments of the nervous system.14 CPGs support our understanding of the rhythmic nature of walking, but this is just one change that is reported by clinicians studying changes in PBWB intervention. Although results vary, changes in step and stride length, base of support, weight shift, hip and ankle kinematics, speed, cardiovascular fitness, and energy expenditure, and, in children, improvements in gross motor skills, have all been reported.13,14,15 These findings are not related to rhythmic movement. Models of MC that stress the interplay of information between the CNS and the body systems shaped by the need to function in specific environmental contexts may be more useful in understanding the overall benefits of this intervention strategy. There is growing evidence that the development of and changes in function, typical or atypical, are linked to neural networks distributed throughout the nervous system, the competencies of all the other body systems, the context, and the task goal, functional context, and dynamical interplay of all these elements.16,17 These newer system-based models, including the theory of dynamic systems (DS) and neuronal group selection (NGS), recognize that, to understand the control of movement, it is equally important to understand the influence and relationships of all the neural and body systems, the specific task that organizes the motor components, and the environmental and sociocultural context within which the action occurs. A more expanded definition looks at the interactions of variables within a single body system; the dynamical, complementary relationships between neural and body systems; the codevelopment of these systems to create constraints and opportunities for adaptive behaviors; and feedback among these systems and their environmental contexts.18 NDT practice currently draws heavily on elements of DS and NGS models conceptualized by Bernstein19 and Edelman,20 respectively. The tenets of these theoretical models have been applied in therapeutic intervention programs for infants, young children, and adults.21,22,23,24,25,26 DS and NGS both emphasize process—how motor behavior occurs and how multiple systems are constrained to create new motor strategies, or to recover from pathology. Both models hypothesize that there is not any one internal system or external context that determines outcome; rather, function is the driving force—functions that have value to the individual and enhance the person’s capacity to carry out meaningful life roles. The primary difference in these two theories is the importance placed on the role of genetically determined neurodevelopmental processes. In NGS, genetic characteristics and experience play equally powerful roles.24 Both models stress the importance of experience and relevance of the context. The relative importance of one system over another will depend on the outcome needed at any given moment to permit continued participation in a changing environment. For the individual to successfully create appropriate and flexible behaviors, there must be intact physical and neural systems and a supportive environment coupled to each other to provide feedback between the body systems and the environment. These theories support NDT assumptions in MC. • Motor behavior emerges from ongoing interactions among multiple internal systems of the individual, the characteristics of the task, and the specific environmental context, each contributing different aspects of MC. • The neural control for movement is distributed throughout various levels of the CNS, all contributing to the final motor outcome. No single site or any one level is responsible for any particular behavior. • Movement is organized around behavioral goals, and function drives the selection of body and neural elements that best meet the needs of the individual. • A hallmark of efficient human motor function is the individual’s ability to select and match a potentially infinite number of movement combinations that are attuned to the forces of gravity, forces generated by the musculoskeletal system, and constraints posed by environmental conditions. • All persons, with or without neuropathology, begin life with a repertoire of movements that, when repeatedly selected and modified by experience and exploration, form the basis for movement combinations designed to meet the needs of the individual throughout the life span. • It is possible to influence a person’s motor behavior by accessing those body systems at times when they are most susceptible to change. Because our clients have an impaired CNS, the next section examines the role of the brain and nervous system, how the brain and nervous system develop and contribute to adaptive behavior, and how neuropathology disrupts this process. Theory of DS contributes most to explaining the importance of experience and the relevance of context, whereas theory of NGS very specifically outlines the role and development of the nervous system as the basis for adaptive behavior. For this reason, this next section uses the theory of NGS to explain organization and role of the nervous system in the process of developing movement. In practice, NDT stresses selecting functional activities outcomes and intervention strategies that match each client’s interests, competencies, and strengths while addressing the client’s impairments that contribute to functional limitations. The theory of NGS, developed by Gerald Edelman,20,27 is one theory that supports this NDT premise. NGS states that (1) as brain structures develop and are organized, they insure that the person has variation in the way he or she can respond to any input, and (2) neural elements can be selected from multitudes of potential possibilities, which are determined by genetic coding and experience, to create individual diversity. These ideas make this theoretical basis consistent with a primary construct of NDT; focus on the individual and his or her needs, abilities, and limitations. A key premise in NGS is the concept of selection. According to Edelman,20 selection is, first, the process by which groups of neurons compete to provide structural diversity in the formation of the anatomy of the brain, and it is also the process which guarantees that the brain and body maintain the conditions for continued life in changing environments. To do this, the brain instantaneously “selects” the response that adapts to external conditions and that is the most fit for each individual person. Inherent in the word selection is the concept that some responses are more fitting than others for the survival and advancement of an individual. NGS places importance on the brain’s ability to select behaviors that are useful and have value to the individual. In this way, NGS differs from DS in that NGS does not assume that a specific organization comes about from random, self-organizing events. Rather, NGS assumes that selection of a particular response pattern is the result of repeatedly selecting and using those neural circuits that the individual needs to build meaningful behaviors. (During embryonic and fetal development this occurs at the cellular and neuroconnectivity level. However, we will assume this same selective process occurs at the behavioral level.) Edelman agrees with other theorists that the brain operates as a dynamic selection system, which implies that selection (of neural pathways or behavioral responses) occurs without a controller. However, in the theory of NGS, the belief is that the neural system is organized by behavior because the behavior has value to the individual. The process is dynamic in that it occurs instantaneously as the individual needs to adapt or change throughout the life cycle and within various environments. The absolute end product of NGS is individual diversity, which states that, within a population, all individuals have common patterns of behavior, such as the way we hold a pencil; greet a friend; respond to stress, joy, or grief; or walk down a slippery slope. Yet all of us have individual differences in how we execute those behaviors based on genetic predispositions, physical differences, contextual experiences, and enormous variation at the levels of neuronal chemistry, network structure, and synaptic strengths.28,29 Individual diversity is what makes each of us interesting and recognizable as individuals. In addition, individual diversity results because each person has different attributes, such as height, age, intellect, coordination, balance, strength, emotional stability, and so on. These individual attributes mean that individuals differ in the ways they respond and adapt to environmental contexts or task conditions. Individual diversity explains why we respond to the same inputs in different ways, the variation in how we benefit from experiences, and why we have different interests and skills and seek different activities. Understanding that there is variability at the neuronal level helps to explain why the expression of CP or stroke varies so much from one client to another. It is not just the location, size of the lesion, or age at which the insult occurs. This concept of individual diversity and all it means is a fundamental idea that NDT therapists consider when they meet new clients, develop a plan of care, and evaluate the success or failure of any specific intervention strategy. Two assumptions of NDT practice are supported by these ideas. 1. NDT therapists respect the differences in every client and plan intervention strategies to target specific system impairments within activities and contexts that are meaningful in the life of the person. 2. Each individual’s behavior is shaped by experience. NDT intervention becomes part of life’s experience, and the NDT therapist has the opportunity to increase the probability that the person will select actions that will allow him or her to effectively solve motor problems. Therapists do this by doing the following: Understanding individual diversity means that we can expect clients to have various ways to move and solve motor problems. The clinician’s role is to identify how we can adapt our intervention to take advantage of the characteristics of the person and fit the intervention to the various system impairments that are standing in the way of solving their functional limitations. We expect previous experiences to impact on the person, and we acknowledge the importance of this as we build intervention strategies. A preterm infant who spent 6 weeks in a neonatal intensive care unit (NICU) with beeping monitors, heel sticks, and medical procedural interruptions might be easily provoked with bright lights, sudden touch, or loud unexpected noise. Intervention strategies may include damping down sensory input so that the infant is not distracted by extraneous information and can focus on important cues to build meaningful movement repertoires. On the other hand, the importance of previous experience can work to the advantage of the therapist. For example, an adult who had many interests and skills prior to stroke, as seen in Case Report A2 describing JW, allows her therapists to draw on a vast array of activities she had been previously engaged in, including gardening, aerobics, canoeing, running, walking her dog, and dragon boat racing, as they planned the intervention. This taps into well-learned and efficient motor memories, uses significant persons in the client’s life, and takes advantage of supportive environments. Diversity helps explain why individuals respond differently to intervention strategies. NDT therapists recognize that what works well for one individual may not work at all for another. Therapists are required to explore various ways to solve any given set of problems, keeping in mind all the systems involved and various avenues for input. Therapists who use the NDT Practice Model do this by observing and analyzing each person’s functional skills and limitations to determine the best choice of intervention strategies for that individual. Intervention is an ongoing, problem-solving approach that leads to the best functional outcomes by minimizing impairments and preventing secondary disability. The therapist expects each client to participate actively in intervention, and, when possible, to take part in goal setting and providing feedback about the effectiveness of various intervention strategies. Although an adult can often provide verbal feedback, therapists need to be sensitive to both verbal and nonverbal feedback from infants, children, and adults. Edelman20,30 states that there are three basic tenets in NGS that describe the following: 1. How the anatomy of the brain arises and takes shape during development, yielding structural variability and primary neuronal repertoires. 2. How experience strengthens and activates certain patterns of response by their adaptive value, yielding secondary repertoires that best fit any given situation. 3. How the resultant maps of the brain are interconnected and give rise to uniquely individual behavioral characteristics in response to environmental demands. Viewed together, these tenets provide solid support for many of the assumptions of NDT intervention; for this reason, each tenet is reviewed in this chapter. These tenets are depicted in Fig. 12.2. Edelman20 proposes that the formation of the basic neuroanatomy of the brain is determined by neural elements—cells, dendrites, and axons and their neurotransmitters. As they compete and connect to other neurons, they have the ability to change the timing, amplitude, and sequences of firing of the neurons they contact. These neural elements are genetically determined and have evolved to both serve the species and impose a set of constraints on the formation of brain structures. In the NGS model, the brain has no wiring diagram; rather, neural structures are determined by the competition among neural elements to assure variation in neuroanatomical structures. Neurons branch in different directions, competing to create immense, variable, and diverse neural circuits. This competition includes cell division, migration, adhesion, death of neurons, and the formation and retraction of synapses that selectively strengthen network connections during fetal development. This competition sets up variation in the basic brain anatomy and sets the stage for uniqueness in responses. In addition, when hundreds of thousands of strongly interconnected neuronal circuits act as structural/functional units, called neuronal groups, they increase their effectiveness. Any single neuron can only be either facilitatory or inhibitory, but when a neuron is part of a neuronal group, the group, because it can change its members, can be facilitatory or inhibitory as needed. In this way, a single neuron can have either facilitatory or inhibitory effects. These structural units or groups, when they function together, form primary motor repertoires. Fig. 12.2 Tenets of the theory of neuronal group selection. Primary motor repertoires are movements characterized by variability and are not connected to either sensory inputs or function (Edelman uses the term primary neuronal repertoires). For our purposes we will refer to these repertoires as primary (and secondary) motor repertoires, because the interest of NDT clinicians is related to motor functions. (For further discussion in these areas, the reader is referred to Edelman’s work.20,27,30) Neural development alone does not explain diversity in primary motor repertoires. At the same time that the nervous system is developing, the sensory system, capable of detecting and recognizing movements that have value to the infant, the musculoskeletal system, and other body systems, develops, resulting in a primary repertoire of species-specific yet unique behaviors. These connected neuronal groups initially develop by genetic instructions and are not tied to the specifics of a situation or feedback from it. But as the fetus develops, they will be affected by signals from the body (exploration in the womb) and eventually by development in an extrauterine environment.26 The resultant primary motor repertoires contain a broad range of movement patterns, which, while they do not yet adapt to the specifics of a situation, have value for survival and the capacity to accommodate and adapt to the environment. This is the basis for providing the infant with a wide range of choices. This very early neural plasticity supports the hypotheses that the brain is a highly dynamic organ capable of structural and functional organization and development in response to internal and external pressures.26,29 Even at birth no two brains are alike, and each infant’s brain is continually changing. The concept of plasticity is an important assumption in the NDT approach as it affects infants, children, and adults. These primary motor repertoires are present at term birth: • Orienting the head and eyes to light and sound. • Orienting the head to clear the airway when prone. • Coordinating suck and swallow. • Bringing the mouth to the hand. • Following moving objects with the eyes. • Projecting the arm toward objects. • Reciprocal kicking. • Sensory elicited reactions and responses (some times referred to as primitive reflexes, such as head and body righting, palmar grasp, rooting reaction, Moro reflex). • General motility. • Attachment to the human face. Initially these primary motor repertoires are characterized by profound variability with considerable degrees of variation in speed, amplitude, participating body parts, and movement direction.26 These early movements appear unrelated to any specific set of conditions. Although all babies have elements of these primary motor repertoires, the expression is highly variable. Some babies appear to be well organized; others do not. The eventual organization and connection between stimulus and action that has value to the infant changes these primary repertoires to secondary through a process called developmental selection, which is discussed under Tenet 2. Primary motor repertoires are basic to the infant’s development, and if they are reinforced by a supportive environment, people in it, and the infant’s success in fulfilling his or her needs, they lead to an even richer, purposeful secondary repertoire of responses. These early interactions between infants and their environment must be coupled with success to reinforce the selection of a particular set of behaviors. This success causes certain neural pathways to be selected and strengthened and results ultimately in infants with diverse ways of expressing needs and wants. If, on the other hand, the infant’s primary motor repertoires are not reinforced, perhaps not intentionally, by caregivers or the environment, and the value of the primary repertoire is lessened, the neural pathway diminishes in strength and brings about a paucity of movement or less variability in the infant’s motor repertoire.31 Edelman30 hypothesizes that, when the brain is in unusual sensory circumstances, events of brain development are modified. For example, think again of the infant in the NICU who might shut down when bombarded with a loud or bright stimulus that has no connection to the infant’s possible motor repertoire. The result may be an infant who cannot link her motor responses to sensory input or continually tries random movement in an attempt to make sense of her sensory world. A premature or sick infant whose attempts to reach out, bring the mouth to the hand, or turn to visual or auditory stimuli, may be so feeble that caregivers do not recognize the relationship between the movement and the intent. Either of these scenarios changes the most primary motor responses and prevents the infant from learning from experience. Als25 reported that infants born prematurely showed more mature fiber structure in the cortex when they received an individualized care program than those who did not. First, NDT clinicians systematically observe and analyze each client’s competencies and limitations to determine the best choice of intervention strategies for that client. Although NDT intervention is directed at both single- and multisystem impairments, which the clinician hypothesizes interfere with the client’s function, the therapist recognizes and respects the differences in each person and the impact that previous experiences have on a client’s posture and movement and responsiveness to various sensory inputs. NDT therapists use a problem-solving approach to plan intervention strategies that are flexible enough to accommodate the differences of each individual client. Case studies in Unit V describe this process. Second, the development of the neuroanatomy by selective competition supports the hypothesis that variability of movement, a hallmark of typical motor development, is established while the brain is developing, and we should expect to see diversity in newborns and young infants. On the other hand, if an insult occurs during fetal development, we can expect to see a reduction of neuronal circuits and therefore a reduction in variation or even loss of primary motor repertoires. One of the major signs of infants with neuropathology is movement that is devoid of variation, complexity, and adaptability.32,33 Therapists can also anticipate that adults who have a sudden onset of neuropathology will in all likelihood exhibit characteristics of primary motor repertoires since these are the first, and most primitive, movement patterns that emerged. This does not mean they demonstrate infantile behaviors, but as the person again attempts complex motor functions, the movements are highly variable and disorganized in spatial, temporal, quantitative, or qualitative aspects. In Case Report A4 of Ernie in Unit V, this 20-year-old with traumatic brain injury (TBI) showed disorganized head, eye, and mouth postures and movements, which improved with intervention. The idea of destabilization is also described as a key concept in DS theory and is viewed as part of the normal developmental process.19,34 Bernstein19 refers to this as a transition state—a time when new movements are most likely to occur. Transitional phases, during which behavior is less stable, are the optimal times to effect changes, providing experiences directed toward functional tasks, structuring the environment, and manipulating control parameters that constrain movement.23,35 For example, as a child with hemiplegia experiences a normal growth spurt at age 2, he may appear clumsy, fall more frequently, stand with more of his weight on the less involved side, or even walk without placing the heel (on the more involved side) on the ground during the stance phase. This is a time to increase the intensity of intervention to take advantage of the variability in gait and balance. Finally, NDT therapists recognize that variability, while inherent in primary motor repertoires, can interfere with organizing more meaningful behaviors. If the individual with CNS impairment practices poorly organized repertoires, this will interfere with the selection and organization of more adaptive responses. NDT therapists use strategies that can help individuals organize their movements in ways that achieve immediate needs and prepare people for more complex functions. We recognize that variability is part of a primary repertoire, and it is important to allow clients, within reason, to select their own way to organize motor responses. Intervention includes assisting the client to organize movement repertoires in relevant contexts. Based on an in-depth knowledge of typical development of the posture and movement systems and changes over time, we set parameters and guide movement to increase the possibility that individuals practice the components of the motor repertoires in ways to assure that eventually they will become part of the individual’s efficient, self-selected, adaptive responses as shown in Case Report B4 in Unit V describing Makayla. In summary, we now have infants with similar yet highly individualized brain structures. This structural variability, developed through competing neural elements, formed primary motor repertoires. The primary repertoires are characterized by profound variability, allowing the infant to explore all motor possibilities within the neurobiological and anthropometric constraints of human development. According to Edelman,30 once primary repertoires have been formed, development proceeds by experiential selection, which combines the primary repertoires with experience in and feedback from external conditions. The transition from primary to secondary repertoires occurs at function-specific ages.36 The product of this second phase is called secondary neuronal repertoires and contains those motor strategies that are the best solutions for a given situation. The second tenet of NGS theory states that the experience of moving, which activates the sensory receptors’ abilities to perceive the effects of various movements in the environment, eventually strengthens or weakens the primary neuronal repertoires. Secondary repertoires of functional circuits develop from the neuronal groups that are part of the primary repertoire of behaviors that have proven to have value for the infant. On a neuronal level, increased synaptic strength or efficacy within a pathway leads to a greater likelihood of conduction across that pathway, whereas decreases in synaptic strength diminish that likelihood.37,38 On a motor level, the more an infant practices a movement repertoire, and gets positive feedback from the movement (value), the more likely the movement is to recur. If there is no value to a movement, the movement drops out of the infant’s repertoire. For example, by 2 months, babies show a specific movement pattern when placed in supine of the head turned to the side (Fig. 12.3). This rather predictable movement is often called the asymmetric tonic neck reflex (ATNR). The movement allows the infant new musculoskeletal experiences—elongation of the pectorals and elbow flexors of the arm on the face side, movement away from physiological flexion seen in newborns, and the option to experience differentiated movement of one upper extremity from the other. In addition, this repertoire connects the hand with the eyes and provides the beginning of a body perceptual experience for the developing infant. At some point, the nervous system starts to use the afferent information provided by the experience for selection of the motor behavior that fits the conditions for exploration. This pattern of movement continues as long as it is useful to the infant. Normally, by 4 months of age, developing infants explore their hands with their eyes in various positions (due to development of antigravity muscles, increased strength, experience, and increased movement repertoires). Although it is still possible to observe the ATNR posture, more variable movements of the extremities are demonstrated that are not tied to movement of the head. This begins the phase of secondary or adaptive variability. This primitive asymmetrical posture can be functional at any age and can be seen when a child or adult must reach outside the base of support (BOS). While making cookies, a 6-year-old girl stands on a small step to reach the counter (Fig. 12.4). She must maintain standing balance on that step as she reaches outside her BOS to decorate her cookies. The predictable asymmetrical posture is accompanied by her head turn and visual attention, aiding her stability. This shift to secondary repertoires is based on active trial-and-error experiences that are unique to the individual. (We will also see that Bernstein19 calls this change a transition or phase shift, an important concept in DS theory.) Three important changes are part of Edelman’s second tenet.20 First, experience changes the strength of neural pathways and their synapses, so that continually experimenting with a particular behavior becomes easier to reproduce when the situation calls for the behavior. Second, the infant organizes postural control as an essential element of all movement repertoires. Third, secondary repertoires link sensory features to specific motor behaviors.
12.1 What Is Motor Control?
12.1.1 Changing Theories of Motor Control
Reflex/Hierarchical Theories
Generalized Motor Program Theory
Central Pattern Generator
12.1.2 How Do These Theories Relate to Clinical Practice?

12.1.3 Models of Motor Control That Emphasize Dynamical Interplay between the Brain, Body, and Environment
12.1.4 NDT Assumptions of Motor Control
12.1.5 Developing Movement Competency
12.1.6 Theory of Neuronal Group Selection
12.1.7 How Does the Idea of Individual Diversity Support NDT?
 Using a problem-solving approach and introducing a wide variety of strategies flexible enough to address the specific system impairments of the individual.
Using a problem-solving approach and introducing a wide variety of strategies flexible enough to address the specific system impairments of the individual.
 Practicing and repeating postures and movements to strengthen the possibility that a particular behavior will occur when the client needs it. For example, in Case Report B6 in Unit V on Jagraj, the therapist described intervention aimed at developing postural stability and tolerance for oral feeding. As he makes progress in both areas, he is able to eat at the table with his family.
Practicing and repeating postures and movements to strengthen the possibility that a particular behavior will occur when the client needs it. For example, in Case Report B6 in Unit V on Jagraj, the therapist described intervention aimed at developing postural stability and tolerance for oral feeding. As he makes progress in both areas, he is able to eat at the table with his family.
 Focusing on the appropriateness and usefulness of the task (or posture and movement) for the individual. Function drives selection of appropriate responses. For example, in Case Report A1 in Unit V describing Mark, a 51-year-old man poststroke, the therapist used his desire to play golf as a way to achieve functional grasp and release, strength, and balance to walk on uneven terrain.
Focusing on the appropriateness and usefulness of the task (or posture and movement) for the individual. Function drives selection of appropriate responses. For example, in Case Report A1 in Unit V describing Mark, a 51-year-old man poststroke, the therapist used his desire to play golf as a way to achieve functional grasp and release, strength, and balance to walk on uneven terrain.
 Using handling in a carefully applied manner to establish or reestablish the postural control and movement components that will enhance temporal, spatial, and force requirements needed for skills.
Using handling in a carefully applied manner to establish or reestablish the postural control and movement components that will enhance temporal, spatial, and force requirements needed for skills.
 Creating a conducive environment, including use of family or other key persons, selecting tools or toys that are reinforcing, and using the therapist–client relationship in a positive way.
Creating a conducive environment, including use of family or other key persons, selecting tools or toys that are reinforcing, and using the therapist–client relationship in a positive way.
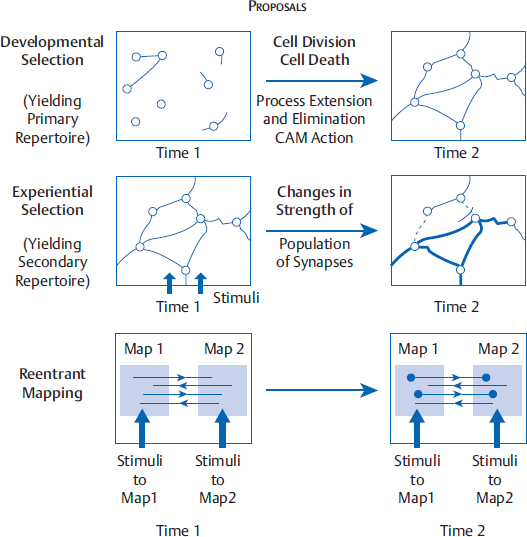
12.1.8 Three Tenets of the Theory of Neuronal Group Selection
Tenet 1: Developmental Selection and Primary Neuronal Repertoires
How Does This First Tenet Support NDT Intervention?
How Do We Apply These Ideas within Intervention?
Tenet 2: Development of Secondary Repertoires of Movement

Related posts:
 The Practice of Speech-Language Pathology from a Neuro-Developmental Treatment Perspective
The Practice of Speech-Language Pathology from a Neuro-Developmental Treatment Perspective
 Report B5 Enhancing Functional Independence in a 10-Year-Old Boy with Cerebral Palsy, Spastic Quadriparesis
Report B5 Enhancing Functional Independence in a 10-Year-Old Boy with Cerebral Palsy, Spastic Quadriparesis
 Report B3 Development of an Intervention Plan of Care for a Young Child with Hemiplegia
Report B3 Development of an Intervention Plan of Care for a Young Child with Hemiplegia
 Neuro-Developmental Treatment Practice Model
Neuro-Developmental Treatment Practice Model
 Report B8 Providing Ongoing Neuro-Developmental Treatment–Based Physical Therapy Intervention for a Medically Fragile Child with Severe Disabilities
Report B8 Providing Ongoing Neuro-Developmental Treatment–Based Physical Therapy Intervention for a Medically Fragile Child with Severe Disabilities
 Neuro-Developmental Treatment Intervention—A Session View
Neuro-Developmental Treatment Intervention—A Session View
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


