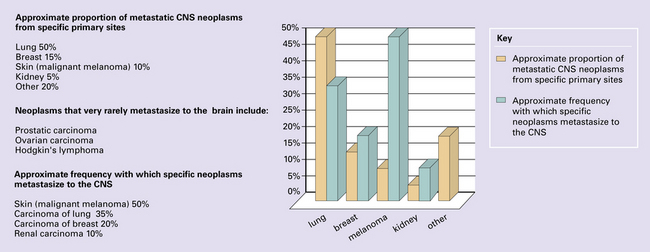
46 Primary neoplasms of the skull and spine may impinge upon the CNS, and (primary) neoplasms in other organs may metastasize to the CNS, its coverings, or its bony surroundings (Fig. 46.1). Neoplasms that spread to the CNS, particularly intracerebral and intravertebral metastases, are common. Their reported incidence varies widely, and reflects whether authors have surveyed necropsy data or clinicopathologic data from centers that deal with different aspects of patient care (neurosurgery, radiotherapy, hospice care). The frequency of CNS metastasis also varies according to the site of primary neoplasm (Fig. 46.1). Primary and secondary neoplasms of the skull and spine produce symptoms and signs by destroying bone and compressing nervous system structures, either elements of the CNS or proximal cranial and spinal nerves (Fig. 46.2). Similar problems are caused on the occasions when mediastinal and retroperitoneal neoplasms invade the extradural space around the spinal cord. Secondary carcinoma is the commonest neoplasm to impinge upon the CNS from surrounding structures, but other types of neoplasm at these sites behave similarly. Diagnosis is facilitated by consideration of the patient’s medical history, assessment of hematologic indices, and a range of imaging studies, in conjunction with histologic examination of biopsies (Figs 46.3–46.5). 46.3 Metastatic carcinoma in the spine. 46.4 Plasmacytic lymphoma (plasmacytoma). 46.5 Chordoma.
Neoplasms that spread to the CNS
 Account for approximately 15% of intracranial neoplasms (in neurosurgical centers).
Account for approximately 15% of intracranial neoplasms (in neurosurgical centers).
 Are eventually present in approximately 30% of patients with disseminated cancer.
Are eventually present in approximately 30% of patients with disseminated cancer.
 Present most frequently in the sixth and seventh decades.
Present most frequently in the sixth and seventh decades.
 Are solitary in approximately 50% of patients.
Are solitary in approximately 50% of patients.
 Are derived most commonly (50% of patients) from primary neoplasms in the lung.
Are derived most commonly (50% of patients) from primary neoplasms in the lung.
 Present before the primary neoplasm in approximately 15% of patients.
Present before the primary neoplasm in approximately 15% of patients.
NEOPLASMS IN TISSUES SURROUNDING THE CNS
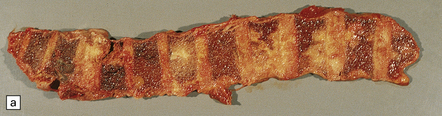
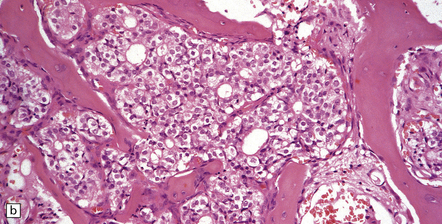
(a) Multiple deposits of metastatic carcinoma are present in the vertebrae. A tumor mass may extend from the bone to compress the spinal cord, but more commonly the pathology causes collapse of the vertebra, which itself compresses the cord. (b) This shows a vertebral deposit of adenocarcinoma from a primary tumor in the prostate gland, which presented with cord compression. An acinar architecture is evident. Common secondary carcinomas in the spine are from primary sites in the breast, lung, and prostate gland. Prostatic carcinoma that has metastasized to bone is commonly osteoblastic, in contrast to metastases from other carcinomas, which tend to be osteolytic. If the origin of a metastatic carcinoma is unknown, immunohistochemistry should be used, along with imaging studies, to investigate possible primary sites; this tumor was immunoreactive for prostatic specific antigen and prostatic acid phosphatase.
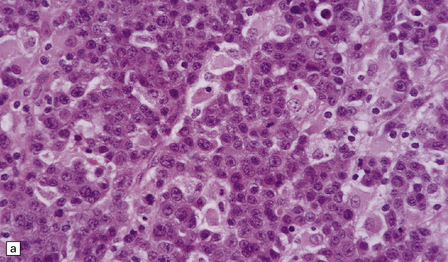
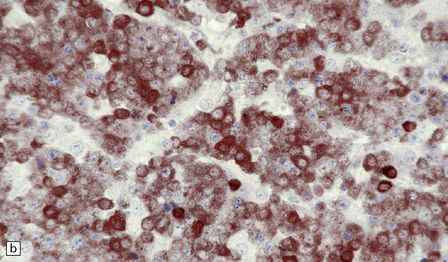
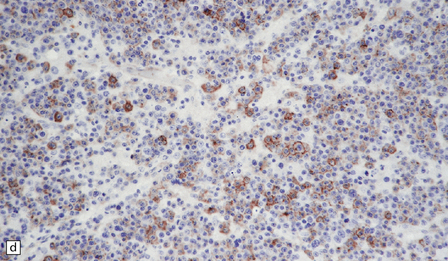
(a) This lymphoreticular neoplasm shows plasma cell differentiation and, in this case, was a solitary lesion in the spine, causing local pain and compression of CNS structures. About 50% of solitary osseous plasmacytic lymphomas progress to multiple myeloma, which is the commonest primary neoplasm within bone to cause CNS symptoms. (b) This plasmacytic lymphoma labeled with an antibody to CD79a, a pan-B cell marker. (c) Light chain restriction can sometimes be demonstrated in plasmacytic lymphoma/multiple myeloma by immunohistochemistry. In this case, cells labeled with a λ antibody (as shown here), but not a κ antibody. In situ hybridization for light chain mRNA is an alternative method for demonstrating clonality. (d) Plasmacytic lymphoma may rarely react with antibodies to epithelial membrane antigen (as shown here), leading potentially to an erroneous diagnosis of metastatic carcinoma. Normal plasma cells are immunoreactive for EMA. CD79a antibodies are helpful in this situation because they should not label carcinomas. With low-grade lymphoid neoplasms comprising well differentiated cells, the issue of whether the pathology is neoplastic or inflammatory sometimes arises. In this situation, establishing immunophenotype or the presence of tumor cell clonality will assist the diagnosis, along with other investigations, such as plasma electrophoresis.
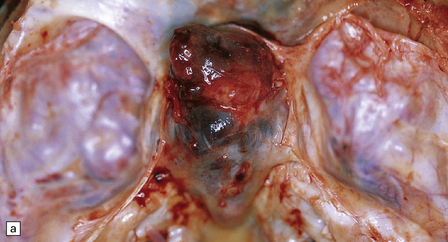
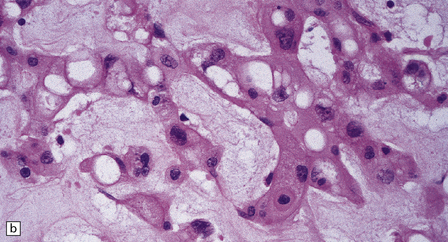
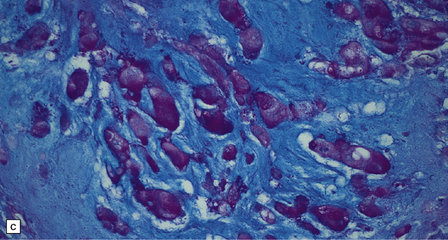
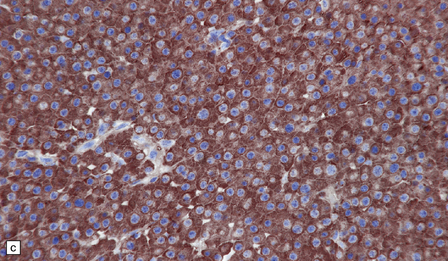
About 80% of chordomas arise in the sacrum or the clivus, growing slowly into the spinal canal or base of the brain respectively. (a) This clival chordoma extends into the pituitary fossa and presented with visual field defects and pituitary dysfunction. The foci of dark gray-brown discoloration are due to hemorrhage at the time of biopsy. (b) The neoplasm consists of strands of cells with vacuolated cytoplasm (physaliphorous cells). (c) The neoplastic cells contain abundant glycogen, stained here with PAS, and are surrounded by a matrix of mucinous, alcianophilic material. A chondrosarcoma may arise in the sacrum or clivus, behaving like a chordoma and showing similar histopathological features. Immunoreactivity for cytokeratins and epithelial membrane antigen can be demonstrated in the cells of a chordoma, but not in the cells of a chondrosarcoma. Immunoreactivity for S-100 protein, which is characteristic of chordomas, helps to differentiate chordoma from metastatic adenocarcinoma.![]()
Stay updated, free articles. Join our Telegram channel
 SECONDARY CNS NEOPLASMS
SECONDARY CNS NEOPLASMS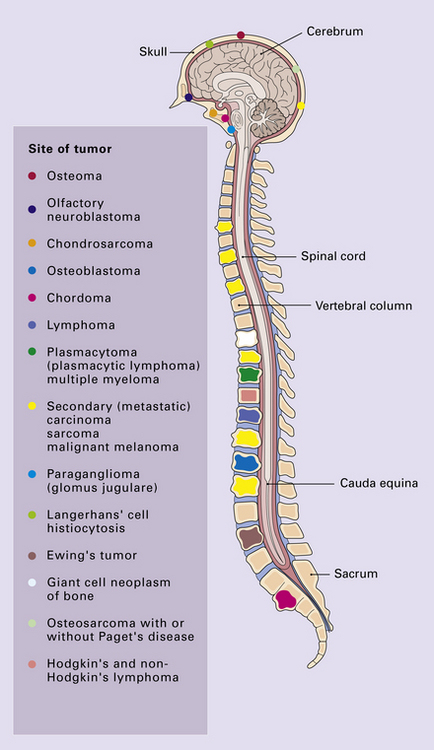



Full access? Get Clinical Tree


