Pedicle Abnormality
Bryson Borg, MD
DIFFERENTIAL DIAGNOSIS
Common
Congenitally Short Pedicles
Stress Reaction
Trauma
Thinning/Remodeling from Intraspinal or Transforaminal Mass
Schwannoma
Neurofibroma
Perineural Root Sleeve Cyst
Arachnoid Cyst
Dural Dysplasia
Meningocele, Lateral
Ependymoma
Destructive Tumor
Metastases, Lytic Osseous
Aneurysmal Bone Cyst
Less Common
Sclerotic/Bone-Forming Tumor
Metastases, Blastic Osseous
Fibrous Dysplasia
Osteoid Osteoma
Osteoblastoma
Osteosarcoma
Osteomyelitis, Granulomatous
Achondroplasia
Congenitally Absent or Hypoplastic Pedicle
ESSENTIAL INFORMATION
Helpful Clues for Common Diagnoses
Congenitally Short Pedicles
Predominately lower lumbar spine
Decreased AP dimension of spinal canal and neural foramina
Stress Reaction
Abnormal biomechanical loading across neural arch, associated with fractures of the pars and pedicle, and degenerative facet disease
Sclerosis (CT) or T2/STIR hyperintensity (MR) ± visible pedicle or pars fracture
Thinning/Remodeling from Intraspinal or Transforaminal Mass
Implies chronic mass effect/slow growth
Cortical margin should be intact on thin-slice bone algorithm CT
Metastases
Often multiple
Thin-slice bone algorithm CT useful to differentiate bony destruction from benign bony remodeling
Purely lytic: Renal, thyroid
Purely sclerotic: Prostate, carcinoid, bladder
Mixed sclerotic &/or lytic: Lung, breast
Helpful Clues for Less Common Diagnoses
Osteomyelitis, Granulomatous
Bony destruction
Epidural/paraspinal abscesses with irregular marginal enhancement
Image Gallery
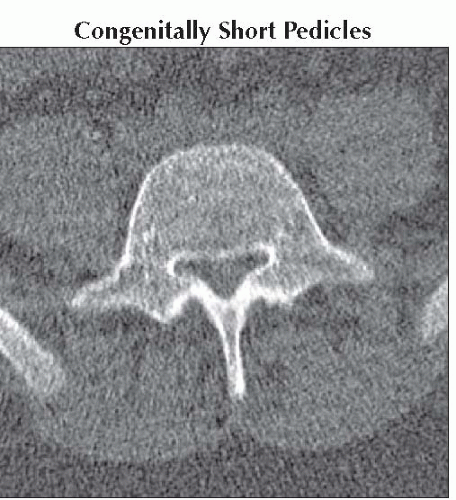 Axial NECT shows a typical case of short lumbar pedicles resulting in congenital spinal stenosis with the characteristic trefoil spinal canal cross section.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|