Polygraphic Recordings
Carlo Alberto Tassinari
Guido Rubboli
Introduction
Polygraphy is a general term that refers to the simultaneous recording of multiple physiologic measures. The main purpose of polygraphic investigations is to provide a correlation between the phenomenology of a behavioral manifestation and a set of physiologic parameters. The polygraphic study must be tailored to each clinical problem to select the parameters relevant to the nature and the characteristics of the manifestation being investigated. Several books and chapters have reported a list of the different variables that can be monitored polygraphically.38,56,104,133
In the study of epilepsy, polygraphy helps to determine the occurrence and characteristics of the modifications of different physiologic functions associated with changes in the electroencephalogram (EEG) and the temporal relationship with the EEG events. Data obtained by means of polygraphy can be extremely useful for describing the symptomatology of epileptic seizures, defining the clinical characteristics of different epileptic conditions, clarifying the physiopathogenetic mechanisms of epileptic conditions, establishing and verifying diagnostic hypotheses, and monitoring and evaluating the action of drugs. This chapter outlines some applications of polygraphic techniques to the study of epilepsy—in particular, its motor manifestations.
Technical Aspects
Currency
Polygraphic recordings are usually performed using modified EEG apparatus. An appropriate number of channels is required, either to collect sufficient information to localize abnormalities or to adequately record polygraphic data. Standard EEG machines usually employ a set of alternating current (AC) amplifiers to collect the data. However, this type of amplifier limits the possibility of recording constant or slowly varying signals (such as those produced by blood pressure, respiratory parameters, or electrodermal resistance). The availability of one or more direct current (DC)-coupled amplifiers can allow the collection of signals whose magnitudes or frequency characteristics range outside those provided by the standard EEG AC machines.
Methodology
The following parameters are relevant to epileptic seizures that can be monitored by means of polygraphic recordings.
Electroencephalogram
Data are collected following the standard procedure for EEG recording. The number of recording channels and the montage used depend on the characteristics of the clinical situation being investigated.
Electromyogram
Surface electromyogram (EMG) activity is obtained by applying two electrodes over the muscular belly of the recorded muscles. To allow collection of high-frequency EMG signals, a short time constant (0.03 second or less) to reduce artifacts caused by movement or sweating and minimum filtering are necessary. Simultaneous EEG and EMG recording can provide useful information to verify the existence of correlations between cortical and muscular events. Analysis of latency between EEG and EMG events, which was once difficult and imprecise by visual inspection of data on paper, can be performed more precisely and reliably by using computerized polygraphic systems that collect the neurophysiologic signals in a digital format and allow off-line processing and analysis of the data. Recording of EMG activity from antigravity muscles can be useful for investigating modification of the muscular tone associated with paroxysmal discharges. Disorders such as tremor or myoclonia require the monitoring of muscular activity of both agonist and antagonist muscle groups.
The inherent limitations of surface EMG, including difficulty recording from a deep or a single muscle without the interference of nearby muscles, loss of high-frequency muscular activity, and inability to obtain single-motor-unit activity, mean that there is only a gross correlation between the EEG and the compound activity of a single muscle. For analysis of the effect of epileptic activity on the single motor unit, needle EMG recording is indicated.
Electrooculogram
Eye movement recording is usually performed by placing two electrodes at the outer canthi to record horizontal movements and one electrode above and the other below one eye to record vertical movements.
When only one electrooculogram (EOG) channel is available, two electrodes can be used, one placed above the outer canthus of one eye and the other placed below the outer canthus of the opposite eye. Other systems have been proposed, including using infrared-detecting cells mounted on a spectacle frame together with an infrared-emitting diod43 or employing piezoelectric sensors.53 Electrooculography is particularly useful for detecting artifacts induced by eye movements, investigating lambda waves, studying ocular manifestations correlated with EEG paroxysms, such as in cases with epileptic nystagmus,58,103 and scoring sleep stages in polysomnography. Computerized methods for removing the EOG artifacts using the EOG signal have been extensively described by Barlow.5
Electrocardiogram
Electrocardiograms (ECGs) can be easily recorded with an EEG device by placing two electrodes on the chest wall or—to obtain a lead I derivation—on the right and left arms. Sensitivity must be adjusted by switching from microvolts per millimeter to millivolts per millimeter; bandwidth ranges from 0.8 to 60 Hz. Simultaneous recording of EEG and ECG allows the detection of pulse and ECG artifacts contaminating the EEG tracing.
Respirogram
Respiratory activity can be monitored either by measuring the changes in thoracic volume due to respiratory movements or by detecting the flow of air through the nostrils and the mouth. Modifications of chest volume can be measured using a strain gauge attached to a piece of elastic forming a band around the chest. Variations of chest circumference due to respiration stretch the elastic band, causing a change in resistance in the strain gauge. Change in resistance can be measured by means of a DC-excited Wheatstone bridge circuit. This system requires that the patient remain still because chest size in moving individuals can change independently from respiration.
Another method for monitoring respiratory activity is to detect the air flow through nostrils and mouth by means of a thermocouple, which generates a current whenever warmed, or by a thermistor, which requires a constant-current source and reproduces changes of temperature as variations of resistance. Both thermocouples and thermistors must be placed between the nostrils and the mouth to detect differences in temperature between inspired and expired air. All of these methods require a long time constant (0.6 or 1 second) and filtering of high frequencies.
Electrodermal Response or Electrodermogram
Electrodermal (EDG) response, also referred to as electrical skin resistance, galvanic skin reflex or response, and psychogalvanic reflex, is a change in resistance and the generation of a potential between areas containing many sweat glands and areas almost devoid of them, due to modifications of sweat gland activity. Change in resistance is also called the Fere effect; the generation of a potential is called the Tarchanoff response. The Fere effect and the Tarchanoff response are probably two measures of the same phenomenon, both being affected by cholinergic modulation.70
Measurement of EDG response is performed by placing one electrode in the palm of the hand or on the sole of a foot and another in an area without sweat glands (such as the back of the hand). Another method is to place both electrodes on the dorsal surface of the forearm 5 to 6 cm apart. Recording must be performed using the longest time constant available with the maximum high-frequency filtering. Measurement of the skin potential, which appears as a DC potential (Tarchanoff response), is quite easy; however, it is unstable due to the possible occurrence of an offset potential at the electrode–skin interface and is difficult to control and distinguish from the EDG. For these reasons, measurement of change in skin resistance is more appropriate.
In normal individuals, resistance recorded from two electrodes on the hand ranges from 20 kΩ to perhaps 0.2 MΩ. If the autonomic nervous system is malfunctioning, resistance can reach values of >1 MΩ. Variations of EDG by measuring the Tarchanoff response during sleep in normal individuals and in patients with epilepsy have been described by Broughton et al.16 Arousal is associated with a decrease in resistance and relaxation with an increase in resistance. Evident EDG modifications were observed—especially during sleep—and were associated with temporal lobe interictal discharges and brief generalized discharges of polyspikes (Fig. 1).
Blood Pressure Monitoring
Blood pressure can be monitored invasively by introducing a microcatheter in the radial artery. The microcatheter is connected with a pressure transducer to polygraph preamplifiers. DC recording is required. It is possible, via microcatheter, to obtain blood samples for blood gas measurements. A preferable method for monitoring blood pressure is a noninvasive assessment based on the computerized processing of instantaneous blood pressure modifications, which are collected by a plethysmographic system applied, usually, to the middle finger of the hand.
Micturition Recorder
A micturition recorder is a device that allows the detection of enuresis or loss of urine due to a convulsive seizure. Broughton37 designed a system consisting of two long electrodes, in separate nylon sheaths, placed parallel with and close to one another in a serpentine shape close to the urinary meatus. The signal recorded, using a high upper-frequency response and a short time constant, is a 50-Hz artifact (60 Hz in North America). As soon as the patient urinates, the first drops of urine create a conductive path between the two electrodes that causes the disappearance of the artifact.
Body Movement Detectors
Systems for signaling body movements are usually based on displacement transducers, accelerometers, or actigraphy monitors. These systems can be applied to the bed of the patient—especially when the aim is to detect seizures during sleep131—or to body parts. A wrist accelerometer can be extremely useful for monitoring movements during sleep,60 identifying different types of movements (tremors, myoclonia),72 and differentiating EEG activity from movement artifacts.18 Actigraphs are small, wrist-worn devices (usually about the size of a wristwatch) that measure movements; they are equipped with a microprocessor and an on-board memory that can allow off-line analysis and display. Actigraphy monitoring is particularly useful in the study of sleep and circadian rhythms.2,64
Gastrointestinal Activity Monitoring
Motility of the gastrointestinal tract was studied by means of EMG recording of the duodenal activity116 using bipolar platinum electrodes. This study investigated modifications of duodenal motility in relation to wakefulness, sleeping (Fig. 2), and ictal activity (Fig. 3). Cherubini et al.20 polygraphic techniques, including monitoring of EMG activity of intestines in cats, to investigate the effects of pharmacologically induced generalized epileptic seizures on intestinal motility.
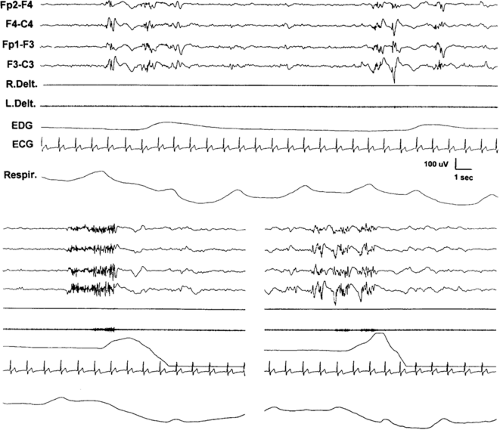 FIGURE 1. Modifications of electrodermogram (EDG) associated with paroxysmal electroencephalogram (EEG) activity during sleep. Upper: Slight EDG changes, indicating a modification of skin potential (Tarchanoff effect), occur as the only manifestation associated with diffuse polyspike-wave activity (note the absence of EMG changes in the deltoids and of modifications of electrocardiogram [ECG] and respiratory rate). Lower: Fast rhythmic activity of polyspikes accompanied by a more significant EDG modification, mild contraction on the left deltoid, and change of respiration. L. Delt, left deltoid; R. Delt., right deltoid; Respir., thoracic respiration. |
Polysomnography in Patients With Epilepsy
The term polysomnography refers to polygraphic recordings of sleep/wake cycle in subjects with sleep disorders. Technical or methodologic aspects of these techniques applied to the study of sleep have been addressed in specialized books and monographs.15,59,61,128 In patients with epilepsy, the role of sleep in facilitating seizures and in activating interictal EEG paroxysmal abnormalities is well known. On the other hand, epileptic seizures can be responsible for modifications of sleep architecture. The relevance of the relationship between epilepsy and sleep has been acknowledged.28,102,132 Sleep polygraphic studies in epilepsy can be extremely useful for diagnosis and for understanding some of the physiopathologic mechanisms of sleep and epilepsy.5a
In epilepsy, polysomnographic studies can be indicated for two reasons: (a) to investigate the presence of disturbances
of vigilance or sleep in patients with epilepsy and (b) to identify and analyze paroxysmal interictal activities, detect nighttime seizures, and evaluate the influence of epilepsy on sleep.
of vigilance or sleep in patients with epilepsy and (b) to identify and analyze paroxysmal interictal activities, detect nighttime seizures, and evaluate the influence of epilepsy on sleep.
Altered alertness in patients with epilepsy can be due to several factors that are either related or unrelated to the epilepsy. Frequent nocturnal seizures altering sleep structure, antiepileptic treatment, and epileptogenic lesions affecting anatomic structures related to vigilance can cause excessive sleepiness in patients with epilepsy. Polysomnographic studies can document the possible occurrence of sleep disorders, such as sleep apnea, and other respiratory disorders, nocturnal myoclonus, or restless leg syndrome.
When the goal of polysomnography is to document nighttime seizures or to investigate the relationship between sleep and epilepsy, a higher number of EEG channels is required than for standard polysomnography. Overnight polysomnography can be helpful to discriminate between epileptic and nonepileptic nocturnal episodes,12,37,49,55,74,77,101,120 characterize and classify nocturnal epileptic seizures,8,75,110 establish the occurrence of electrical status epilepticus during sleep,107,108 identify the primary focus in localization-related epilepsy by investigating topography of paroxysms during rapid-eye-movement (REM) sleep,71,89 and analyze the behavior of interictal discharges during sleep.8,25,27,33,36,66,84,125,126
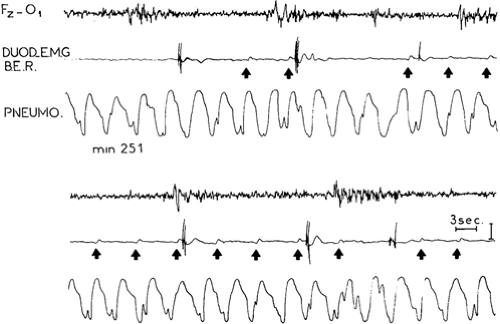 FIGURE 2. Sleep polygraphic tracing with duodenal electromyogram (EMG) recording in a normal individual. Basal electrical activity can be associated with bursts of muscular potentials accompanying duodenal contractions (arrows). No constant relation is observed between duodenal electrical activity and K complexes. DUOD E.M.G. BER, duodenal EMG demonstrating basal electrical activity; PNEUMO., respirogram. |
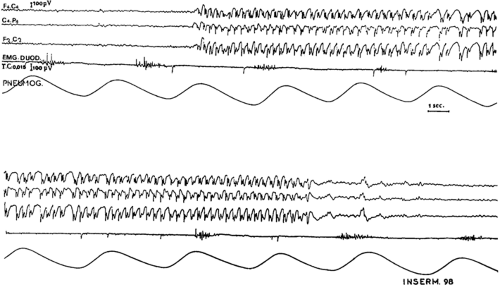 FIGURE 3. Duodenal electromyogram (EMG. DUOD.) activity persisted unmodified (or, possibly, slightly decreased) during spike-and-wave discharges; PNEUMOG., respirogram. |
Polygraphic Studies in the Investigation of Epileptic Motor Manifestations
Motor phenomena are often the most overt clinical aspects of an epileptic seizure. However, when one is relying solely on clinical data, the patterns of muscular activations can be difficult to characterize and analyze. Mild contractions or sporadic muscle twitchings can often be missed by an observer. Polygraphy with recording of surface EMG activity can be extremely
useful in identifying and characterizing even subtle and apparently subclinical muscular manifestations and correlating these movements with EEG activities.
useful in identifying and characterizing even subtle and apparently subclinical muscular manifestations and correlating these movements with EEG activities.
Analysis of Motor Phenomenon
Surface EMG recording can provide information regarding the modality of muscular contraction, which can allow distinctions to be made among different types of motor phenomenon. All of the following types of muscular phenomena can occur, either in isolation or in various combinations, to constitute the clinical manifestations of the different types of epileptic seizures.
Myoclonus
A positive myoclonus is characterized by a massive, shock-like muscular contraction involving one or more body segments. It appears in the EMG as a brief burst of muscular potentials (Fig. 4), synchronous on agonist and antagonist muscles, with or without an EEG correlate. The opposite phenomenon, a “negative” myoclonus, is a brief interruption of a tonic muscular contraction (Fig. 4), sometimes clinically indistinguishable from the positive myoclonus.94,123 When associated with a paroxysmal EEG event, a negative myoclonus is defined as “epileptic negative myoclonus” (Fig. 5).48,106,122 Negative myoclonus, defined as an interruption of tonic muscular activity for <500 msec without evidence of preceding myoclonia, was recognized in 2001 as a seizure type by the Task Force of the International League Against Epilepsy on Classification and Terminology.13
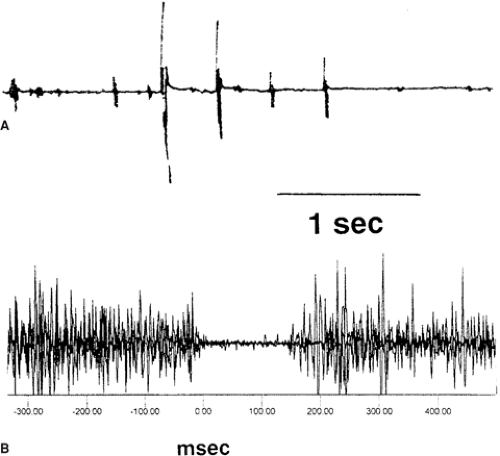 FIGURE 4. A: Positive myoclonus. B: Negative myoclonus. |
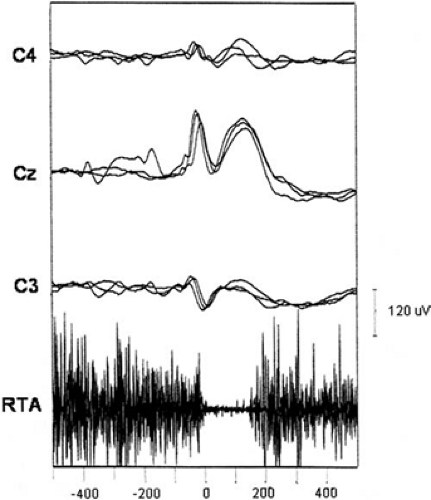 FIGURE 5. Epileptic negative myoclonus. Superposition of three polygraphic segments illustrating a spike-wave complex on Cz, slightly spreading to C3 and C4, associated with epileptic negative myoclonus in right tibialis anterior (RTA), in a child with benign partial epilepsy of infancy. The onset of the electromyogram silent period in RTA precedes the onset of the slow-wave component on Cz, suggesting that the muscular inhibition is related to the spike and not to the slow wave. |
Spasm
A spasm, which appears as a massive but slow contraction reaching a climax and progressively decreasing, more often than not involves axial and proximal muscular groups. Indeed, polygraphic recordings with multiple EMG leads have demonstrated that epileptic spasms can occur with a complex pattern of muscular activation, with the involvement of cranial as well as limb and axial muscles. This complex pattern of contraction can appear clinically similar in different spasms, although with variable sequences of muscular recruitment (Fig. 6).10,134 On the EEG, spasms can be devoid of any modification of tracing or they can be associated with flattening, diffuse low-voltage fast activity,42 or a slow wave.34,46
Tonic Contractions
Tonic contractions consist of slow, sustained contractions maintained over time and involving several muscular groups. They are usually associated with fast recruiting EEG activity.
Clonic Contractions
Clonic contractions are characterized by a series of jerks, appearing on the EMG as hypersynchronous muscular potentials. They can vary in amplitude, symmetry, frequency, and topography and are often related to contralateral EEG spikes.42
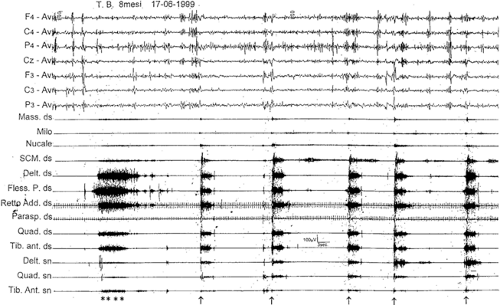 FIGURE 6. Polygraphic recording of a cluster of spasms (arrows) following a brief tonic seizure (asterisks) in an 8-month-old child with severe epileptic encephalopathy associated with cortical dysplasia. The multichannel electromyogram recording shows the involvement of cranial, trunk, and limb muscles with a quite reproducible pattern. A slow complex associated with the spasms is detectable in the electroencephalogram (horizontal time scale: 3 s). Delt., deltoid; ds, right; Fless. P., wrist flexor; Mass., masseter; Milo, mylohyoideus; Nucale, splenium capitis; Parasp, paraspinal muscles; Quad., quadriceps; Retto Add., rectus abdominis; SCM., sternocleidomastoideus; sn, left; Tib.ant., tibialis anterior. |
Atonic Phenomena
Atonic phenomena can appear as a sudden global or focal loss of muscular tone, characterized polygraphically by an abrupt flattening of the EMG activity. They are associated with different types of EEG paroxysmal discharges (generalized spike- or polyspike-and-wave, diffuse fast rhythmic spikes, bilateral synchronous fast waves intermixed with slow waves) or with no EEG changes at all.42
Analysis of Motor Pattern
Polygraphy can be extremely relevant for defining the characteristics of a motor manifestation during a seizure in terms of (a) the relationship with the concomitant EEG activity, (b) muscular groups involved in the seizure, (c) the temporal succession and the time course of the activation of motor patterns during the seizure, and (d) the presence of a stereotypic motor pattern across different seizure types.
Generalized Tonic–Clonic Seizures
Polygraphic recordings make it possible to characterize the complex manifestations of generalized tonic–clonic seizures, which are composed of a more or less stereotyped sequence of motor phenomena.9,29,38,40 This sequence consists of an initial tonic phase of sustained muscular contraction lasting 10 to 20 seconds and involving all skeletal muscles. This phase is responsible for the characteristic body attitude (a flexion followed by a longer extension phase). A diffuse vibratory contraction follows this initial phase, and clonic manifestations follow next. The clonic manifestations consist of brief, maximal flexor contractions of the whole body, with the interval between the jerks becoming progressively longer. It is interesting that polygraphic recordings have demonstrated that, just a few seconds after the last clonic jerk, a new tonic phase usually reappears, as intense as the first one but with different topographic distribution, involving mainly facial and masticatory muscles.42
The EEG correlates of a tonic–clonic seizure are usually represented by an initial desynchronization, sometimes preceded by generalized bursts of polyspike-and-waves, followed by a recruiting rhythm. These are intermixed with slow waves of decreasing frequency and increasing amplitude that correspond, at a certain point, with the interruption of the tonic massive contraction and with the onset of the clonic manifestations. A flattening of the EEG activity follows, which represents the phase of “cortical extinction” and lasts several seconds (see Chapters 47 and 74).
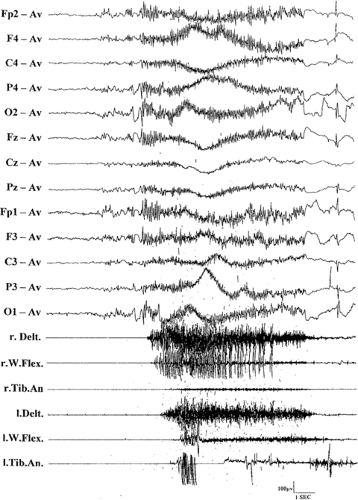 FIGURE 7. Tonic seizure. The bilateral tonic contraction, more prominent in both deltoids, is associated with a fast rhythmic polyspike activity. Delt., deltoid; l, left; r., right; Tib. An., tibialis anterior; W. Flex., wrist flexor. |
Tonic Seizures
Clinical features of tonic seizures consist of a brief (5 to 20 seconds) muscular tonic contraction accompanied by impairment of consciousness and involving, with varying degrees of intensity and extension, distinct muscular groups (i.e., the head and trunk or the limb girdles and, to a lesser extent, the legs) or the whole body.19,40,41,42 The associated polygraphic findings are represented by different EEG patterns such as (a) flattening of the tracing, (b) fast activity (around 20 Hz) of progressively increasing amplitude, and (c) recruiting rhythmic discharge at about 10 Hz, sometimes of high amplitude from the onset. The EMG leads show an interference pattern in all involved muscles corresponding to the tonic contraction (Fig. 7). Different
patterns of muscular activation can be observed according to the duration of the seizure: When it lasts a short time, the contraction is maximal at the onset, then decreases; when it is of longer duration, a progressive increment of the muscular activity reflects the increasing intensity of the contraction. In global tonic seizures, an axial preponderance of the muscular activation is evident. Asymmetry of the tonic contraction or the occurrence of myoclonia at the end of the tonic manifestation can be observed. Tonic seizures are often associated with autonomic changes, such as modifications of heart and respiration rate, mydriasis, vasomotor phenomena, increase in intravesicular pressure, and positive electrodermogram responses (see Chapter 52).19,40
patterns of muscular activation can be observed according to the duration of the seizure: When it lasts a short time, the contraction is maximal at the onset, then decreases; when it is of longer duration, a progressive increment of the muscular activity reflects the increasing intensity of the contraction. In global tonic seizures, an axial preponderance of the muscular activation is evident. Asymmetry of the tonic contraction or the occurrence of myoclonia at the end of the tonic manifestation can be observed. Tonic seizures are often associated with autonomic changes, such as modifications of heart and respiration rate, mydriasis, vasomotor phenomena, increase in intravesicular pressure, and positive electrodermogram responses (see Chapter 52).19,40
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


