Chapter 3 Radiologic Anatomy of the Spine
The cervical spine
Atlas (C1)
The lateral masses consist of superior and inferior articular facets and transverse processes. The superior articular facets are concave and ovoid, and they face upward and inward as shallow foveae for articulation with the occipital condyles. Nutatory movements of the head mainly occur at these atlantooccipital joints. The inferior articular facets are concave and face downward, slightly medially, and backward; they articulate with the superior articular facets of the axis. The relative horizontal orientation of the atlantoaxial facet joints allows rotation at the expense of bony stability. The paired alar ligaments, running from the posterolateral aspects of the odontoid process to the occipital condyles, prevent excessive rotation [1]. The transverse processes are each pierced by a foramen for the vertebral artery. On coronal CT scans, the occipitoatlas and the atlantoaxial joints resemble a capital X.
C3 to C7 Vertebrae
Vertebral Bodies
The vertebral bodies in the cervical spine are ladder-like in cross section; they are broader in the transverse diameter than in the anteroposterior (AP) dimension, and their end plates are parallel (Fig. 3-1). The cervical vertebral bodies are smaller than those of the other movable vertebrae and increase in size from C3 downward. The vertebrae are connected by the anterior and posterior longitudinal ligaments. Each ligament’s fibers diverge at each disc level and blend with the anulus fibrosus and the adjacent margins of the vertebral bodies. At the mid-vertebral level, the posterior longitudinal ligament is narrower and lies behind the body, posterior to the retrovertebral venous plexus.

Joints of von Luschka
The upper and lateral edges of the superior surface project upward and have sagittal ridges that form the uncinate processes. Together with corresponding notches in lower end plates of the vertebra above, they form the uncovertebral joints of von Luschka (Fig. 3-2).

Transverse Foramen
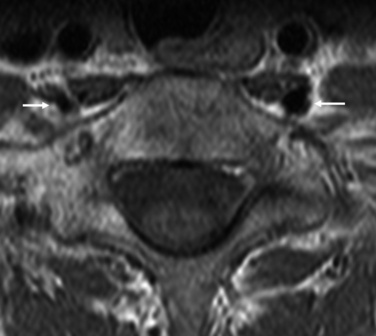
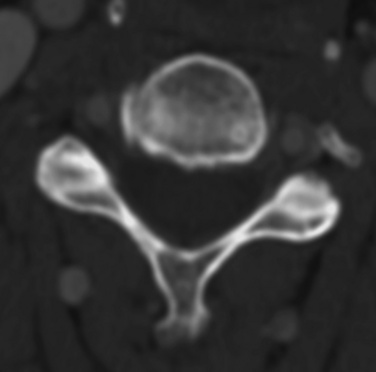
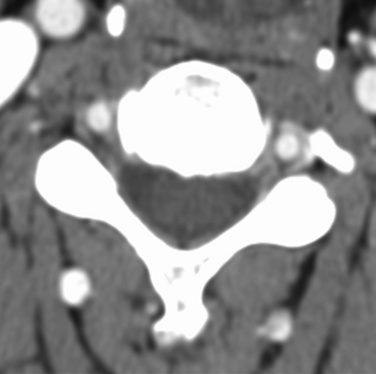
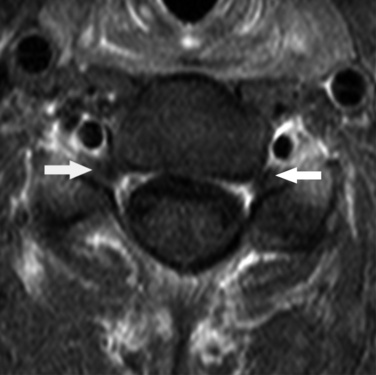
The transverse foramen, a characteristic feature of the cervical spine, houses the vertebral artery, veins, and sympathetic nerves in the deep cranial groove of the transverse process. The spinal nerves and ganglia cross the dorsal border of the artery along with segmental vessels. The transverse foramen of the seventh cervical vertebra contains only vertebral veins, not the vertebral artery (Figs. 3-3 and 3-4).
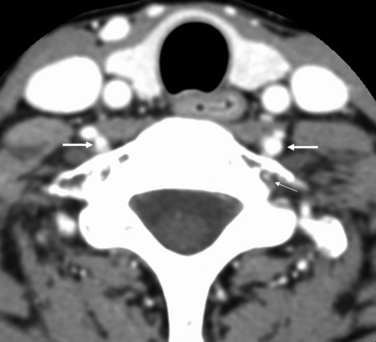
Figure 3–3 Axial CT scan of the seventh cervical vertebra. The transverse foramen of the seventh cervical vertebra contains only vertebral veins (thin arrow), not the vertebral artery (thick arrows). However, the other cervical vertebrae contain the vertebral artery within their transverse foramina. See also Fig. 3-4.
Articular Processes
The superior and inferior articular processes of adjacent neural arches form the facet joints. These structures are more oblique in the cervical level than in other levels of the spine. Each joint surface is lined with articular cartilage, and menisci cushion the cervical facets. Surrounding each joint is a fibrous capsule with a synovial membrane on its inner aspect; this capsule is relaxed to allow a gliding motion. Anteriorly, the superior articular facet is rounded in its anterior aspect; its articular surface faces posteriorly and is flat. Posteriorly, the inferior articular facet of the vertebra above has a flat anterior articular surface and a convex posterior aspect (Fig. 3-5).
Spinal Canals
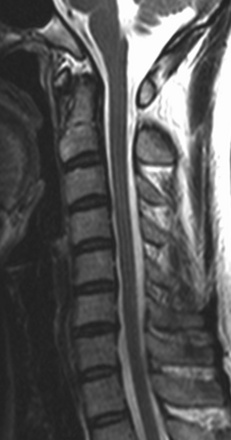
The spinal canals are relatively large in order to house the cervical enlargement of the spinal cord. The spinal canal is triangular with the apex of the triangle posterior. The canal decreases in size from vertebra C1 through vertebra C3 and has a fairly uniform dimension from C3 through C7. C7 is a transitional vertebra, whose spinous process is longer and thicker and has a more inferior tilt than the more rostral cervical spinous processes of C3 to C6. On a T1-weighted MR image, the exact size of the subarachnoid space is difficult to assess because of its low signal intensity, and it may be confused with the posterior longitudinal ligament and the cortical bone (Fig. 3-6).

Epidural Space
The epidural space that surrounds the dural sac contains neurovascular and connective tissue elements that are more clearly seen on MRI and CT after intravenous injection of a contrast agent. There is only a small amount of epidural fat tissue, and sinuses are formed in this fat tissue by the wide venous plexuses that surround roots and nerves as they leave the intervertebral foramina in the lateral parts of the epidural space (Fig. 3-7). The scarcity of revised epidural fat in the cervical canal in comparison with that in the lumbar canal makes it more difficult to differentiate between the soft tissue structures in the cervical spinal canal on a noncontrast CT scan. On MRI, the high signal intensity in the anterior lateral aspect of the cervical canal represents the epidural venous plexus. The epidural venous plexuses produce high signal intensity in the anterior epidural space, which should not be confused with epidural fat; epidural fat is virtually absent at the cervical level.
Cervical Discs
The cervical intervertebral discs are smaller than the discs of other regions of the spine. The uncinate processes on the upper end plate limit lateral extension of the discs. These discs are wedge-shaped, the greater width being anterior, corresponding to the cervical lordosis [2]. The intervertebral discs do not extend anteriorly or posteriorly beyond the level of the vertebral body in younger people. The nucleus pulposus cannot be differentiated from the anulus fibrosus, but the periphery of the disc is less intense than its central portion. (Figs. 3-6 and 3-8).
Nerves of the Cervical Cord
Spinal nerves arise from the cervical cord. Each nerve consists of a dorsal sensory root and a ventral motor root. The nerve roots join just lateral to the dural sheath to form the spinal nerves. The dorsal root ganglion is located in the neural foramen just proximal to the point of union of the dorsal and ventral roots. The roots of each spinal nerve from C1 through C7 leave the spinal canal through the intervertebral foramina above the corresponding vertebra. The eighth cervical nerve passes through the foramen between C7 and T1. The spinal ganglion, located outside and below the neural foramen, is clearly seen posterior to the vertebral artery on MRI as a structure of intermediate signal intensity. On contrast-enhanced MR images, the spinal ganglion appears as a mildly enhancing ovoid structure posterior to the vertebral artery (Fig. 3-9).
Related posts:
 Lateral Interbody Fusion Using the XLIF System
Lateral Interbody Fusion Using the XLIF System
 Percutaneous Lumbar Restabilization via a Posterolateral Approach
Percutaneous Lumbar Restabilization via a Posterolateral Approach
 Anterior Endoscopic Cervical Microdecompression of Disc and Foramen
Anterior Endoscopic Cervical Microdecompression of Disc and Foramen
 Outcome Measurements for Minimally Invasive Percutaneous Spine Techniques
Outcome Measurements for Minimally Invasive Percutaneous Spine Techniques
 Spinal Cord Stimulation
Spinal Cord Stimulation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


