12
Seizures & Syncope
EPISODIC LOSS OF CONSCIOUSNESS
Consciousness is lost when the function of both cerebral hemispheres or the brainstem reticular activating system is compromised. Episodic dysfunction of these anatomic regions produces transient, and often recurrent, loss of consciousness. There are two major causes of episodic loss of consciousness.
SEIZURES
Seizures are disorders characterized by temporary neurologic signs or symptoms resulting from abnormal, paroxysmal, hypersynchronous electrical neuronal activity in the cerebral cortex.
SYNCOPE
Syncope is loss of consciousness due to a reduced supply of blood to the cerebral hemispheres or brainstem. It can result from pancerebral hypoperfusion caused by vasovagal reflexes, orthostatic hypotension, or decreased cardiac output or from selective hypoperfusion of the brainstem resulting from vertebrobasilar ischemia.
It is important to distinguish seizures from syncope because they have different causes, diagnostic approaches, and treatment.
APPROACH TO DIAGNOSIS
The initial step in evaluating a patient who has suffered a lapse of consciousness is to determine whether the setting in which the event occurred, or associated symptoms or signs, suggests that it was a direct result of a disease requiring prompt attention, such as hypoglycemia, meningitis, head trauma, cardiac arrhythmia, or acute pulmonary embolism. The number of spells and their similarity or dissimilarity should be established. If all spells are identical, then a single pathophysiologic process can be assumed. The following major differential features should be ascertained.
EVENTS AT ONSET OF SPELL
Prodromal Symptoms (Aura)
A detailed inquiry should always be made about prodromal and initial symptoms. A witness is critical. The often brief, stereotyped premonitory symptoms (aura) at the onset of some seizures may localize the central nervous system (CNS) abnormality responsible for seizures. Note that more than one type of aura may occur in a given patient.
Posture When Loss of Consciousness Occurs
Orthostatic hypotension and simple faints occur in the upright or sitting position. Episodes that also or only occur in the recumbent position suggest seizure or cardiac arrhythmia as a likely cause, although syncope induced by strong emotional stimuli (eg, phlebotomy) can also occur in recumbency.
Relationship to Physical Exertion
Syncope induced by exertion is usually due to cardiac outflow obstruction (eg, aortic stenosis, obstructive hypertrophic cardiomyopathy, atrial myxoma) or arrhythmias.
Focal Motor or Sensory Symptoms
Focal motor or sensory phenomena (eg, involuntary jerking of one hand, hemifacial paresthesias, or forced head turning) suggest a seizure originating in the contralateral frontoparietal cortex.
Affective or Cognitive Symptoms
A sensation of fear, olfactory or gustatory hallucinations, or visceral or déjà vu sensations are commonly associated with seizures originating in the temporal lobe.
Presyncopal Symptoms
Progressive light-headedness, dimming of vision, and faintness, which indicate diffuse CNS dysfunction, are associated with decreased cerebral blood flow (eg, simple faints, cardiac arrhythmias, orthostatic hypotension).
EVENTS DURING THE SPELL
Tonic Stiffening and Clonic Movement
Generalized tonic–clonic (grand mal, or major motor) seizures are characterized by loss of consciousness, accompanied initially by tonic stiffening and subsequently by clonic (jerking) movements of the extremities.
Flaccidity
Cerebral hypoperfusion usually produces flaccid unresponsiveness.
Brief Stiffening or Jerking
Cerebral hypoperfusion can also result in stiffening or jerking movements, especially if hypoperfusion is prolonged because the patient is prevented from falling or otherwise assuming a recumbent posture. This phenomenon, sometimes referred to as convulsive syncope, is self-limited and does not require anticonvulsant treatment. Loss of consciousness from hypoperfusion rarely lasts more than 10 to 20 seconds and is not followed by postictal confusion unless severe and protracted brain ischemia has occurred.
EVENTS AFTER THE SPELL
Prompt Recovery of Consciousness
Recovery from a simple faint is characterized by a prompt return to consciousness, with full lucidity, within 20-30 seconds.
Brief Confusion
A period of confusion, disorientation, or agitation (postictal state) follows a generalized tonic–clonic seizure. The period of confusion usually lasts only minutes. Although such behavior is often strikingly evident to witnesses, it may not be recalled by the patient.
Prolonged Confusion
Prolonged alteration of consciousness (prolonged postictal state) may follow status epilepticus. It may also occur after a single seizure in patients with diffuse structural cerebral disease (eg, dementia, other cognitive impairment, or encephalitis) or metabolic encephalopathy.
Tongue Biting
Biting of the lateral aspect of the tongue is highly specific for generalized tonic–clonic seizure and may be noted by the patient after such a spell.
Urinary Incontinence
On regaining consciousness, patients may discover that they have been incontinent of urine, but this can occur during either seizure or syncope. Fecal incontinence is uncommon.
SEIZURES
A seizure is a transient disturbance of cerebral function caused by an abnormal neuronal discharge. Epilepsy, a group of disorders characterized by recurrent seizures, is a common cause of episodic loss of consciousness; the prevalence of epilepsy in the general population is about 1%, and the lifetime probability of a seizure is approximately 10%.
An actively convulsing patient or a reported seizure in a known epileptic usually poses no diagnostic difficulty. However, because most seizures occur outside the hospital unobserved by medical personnel, the diagnosis often must be established retrospectively. The two historic features most suggestive of a seizure are the aura associated with seizures of focal onset and the postictal confusional state that follows generalized tonic–clonic seizures (see later).
ETIOLOGY
Seizures can result from either primary CNS dysfunction or an underlying metabolic derangement or systemic disease. This distinction is critical, because therapy must be directed at the underlying disorder as well as at seizure control. A list of common neurologic and systemic disorders that produce seizures is presented in Table 12-1. The age of the patient may help in establishing the cause of seizures (Figure 12-1).
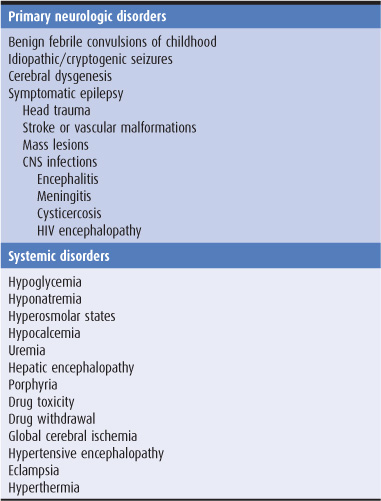
Table 12-1. Common causes of seizures of new onset.
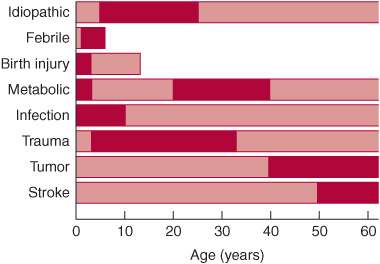
Figure 12-1. Causes of seizures as a function of age at onset. Bars show the range of ages at which seizures from a given cause typically begin; darker shading indicates peak incidence.
The genetic contribution to epilepsy and its response to treatment is complex. A single epileptic syndrome (eg, juvenal myoclonic epilepsy) can result from mutations in several different genes and, conversely, mutations in a single gene (eg, SCN1A sodium channel subunit) can cause several epilepsy phenotypes. Genes implicated in susceptibility to epilepsy include those coding for sodium, calcium, potassium, and chloride channels; nicotinic cholinergic, GABA, and G protein-coupled receptors; and enzymes.
PRIMARY NEUROLOGIC DISORDERS
Benign Febrile Convulsions
Benign febrile convulsions occur in 2% to 5% of children aged 6 months to 5 years, usually during the first day of a febrile illness (temperature > 100.4°F or 38°C), and in the absence of CNS infection (meningitis or encephalitis). There may be a family history of benign febrile convulsions or other types of seizures. Mutations in several genes have been linked to febrile convulsions, including the G protein-coupled receptor MASS1; the inositol monophosphatase IMPA2; SCN1A, SCN1B, and SCN2A sodium channel subunits; KCNQ2, KCNQ3, and KCNA1 potassium channel subunits; and GABRG2 and GABRD GABA receptor subunits.
Benign febrile convulsions usually last for less than 10 to 15 minutes and lack focal features. Approximately two-thirds of patients experience a single seizure, and fewer than one-tenth have more than three. Seizures occurring during the first hour of fever in children younger than 18 months or in children with a family history of febrile seizures are associated with an increased risk for recurrence; 90% of recurrences occur within 2 years of the initial episode. The differential diagnosis includes meningitis and encephalitis (Chapter 4); if present, these should be treated as described elsewhere in this volume.
Because benign febrile convulsions are usually self-limited, treatment is often unnecessary; prolonged convulsions (≥15 minutes) can be treated with diazepam 0.3 mg/kg orally, intramuscularly, or intravenously or 0.6 mg/kg rectally. Such treatment may decrease the risk of recurrence. The probability of developing a chronic seizure disorder is 2% to 6% and is highest in patients with persistent neurologic abnormalities; prolonged, focal, or multiple seizures; or a family history of nonfebrile seizures. Long-term administration of phenobarbital to reduce the risk of subsequent afebrile seizures is rarely indicated, as the risk of nonfebrile seizures is not altered.
Idiopathic (Cryptogenic) Seizures
These account for two-thirds of new-onset seizures in the general population. The age range is broad, from the second to the seventh decade (Figure 12-1). The risk of recurrence in the next 5 years is approximately 35% after a first unprovoked seizure. A second seizure increases the risk of recurrence to approximately 75%. Most recurrences occur in the first year. Genes implicated in idiopathic generalized epilepsy include the mitochondrial NAD-dependent malic enzyme ME2 and the CACNA1A and CACNB4 calcium channel subunits.
Head Trauma
Head trauma is a common cause of epilepsy, particularly when it occurs perinatally or is associated with a depressed skull fracture or intracerebral or subdural hematoma. Seizures that occur within the first week after nonpenetrating head injuries are not predictive of a chronic seizure disorder, however. Although patients with serious head injuries are often treated prophylactically with anticonvulsant drugs, this practice has been questioned, because a reduction in the incidence of posttraumatic seizures has not been consistently observed.
Stroke
Stroke affecting the cerebral cortex produces seizures in 5% to 15% of patients and can occur after thrombotic or embolic infarction or intracerebral hemorrhage (Chapter 13). As in head trauma, early seizures are not necessarily indicative of chronic epilepsy, and long-term anticonvulsant therapy may not be required. Even without rupturing, vascular malformations may be associated with seizures, presumably as a result of their irritative effects on adjacent brain tissue.
Mass Lesions
Mass lesions, such as brain tumors (Chapter 6) or abscesses (Chapter 3), can present with seizures. Glioblastomas, astrocytomas, and meningiomas are the most common tumors associated with seizures, reflecting their high prevalence among tumors that affect the cerebral hemispheres.
Meningitis or Encephalitis
Bacterial (eg, Haemophilus influenzae or tuberculous), viral (eg, herpes simplex), fungal, or parasitic (eg, cysticercosis) infections (Chapter 4) can also cause seizures. Seizures in patients with AIDS are most often related to HIV-associated dementia, but also occur with toxoplasmosis or cryptococcal meningitis.
Developmental Anomalies
Cortical dysgenesis and neuronal migration disorders can predispose to epilepsy.
SYSTEMIC DISORDERS
Metabolic and other systemic disorders, including drug-overdose and drug-withdrawal syndromes, may be associated with seizures that abate with correction of the underlying abnormality. In these cases, the patient is not considered to have epilepsy.
1. Hypoglycemia (Chapter 4) can produce seizures, especially with serum glucose levels of 20 to 30 mg/dL, but neurologic manifestations of hypoglycemia are also related to the rate at which serum glucose levels fall.
2. Hyponatremia (Chapter 4) may be associated with seizures at serum sodium levels less than 120 mEq/L or at higher levels after a rapid decline.
3. Hyperosmolar states, including both hyperosmolar nonketotic hyperglycemia (Chapter 4) and hypernatremia, may lead to seizures when serum osmolality rises above approximately 330 mOsm/L.
4. Hypocalcemia (Chapter 4) with serum calcium levels in the range of 4.3 to 9.2 mg/dL can produce seizures with or without tetany.
5. Uremia (Chapter 4) can cause seizures, especially when it develops rapidly, but this tendency correlates poorly with absolute serum urea nitrogen levels.
6. Hepatic encephalopathy (Chapter 4) is sometimes accompanied by generalized or multifocal seizures.
7. Porphyria is a disorder of heme biosynthesis that produces both neuropathy (Chapter 9) and seizures. The latter may be difficult to treat because most anticonvulsants can exacerbate the metabolic abnormalities. Case reports attest to the safety and efficacy of gabapentin, oxcarbazepine, and levetiracetam in porphyria.
8. Drug overdose can exacerbate epilepsy or cause seizures in nonepileptic patients. Generalized tonic–clonic seizures are most common, but focal or multifocal partial seizures can also occur. The drugs most frequently associated with seizures are antidepressants, antipsychotics, cocaine, insulin, isoniazid, lidocaine, and methylxanthines (Table 12-2).
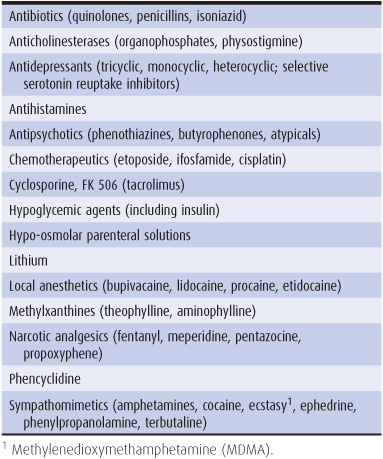
Table 12-2. Major categories of drugs reported to cause seizures.
9. Drug withdrawal, especially withdrawal from ethanol or sedative drugs (Chapter 4), may be accompanied by one or more generalized tonic–clonic seizures that usually resolve spontaneously. Alcohol withdrawal seizures occur within 48 hours after cessation or reduction of ethanol intake in 90% of cases and are characterized by brief flurries of one to six attacks that resolve within 12 hours. Acute abstinence from sedative drugs can also produce seizures in patients habituated to more than 600 to 800 mg/d of secobarbital or equivalent doses of other short-acting sedatives. Seizures from sedative drug withdrawal typically occur 2 to 4 days after abstinence but may be delayed for up to 1 week. Focal seizures are rarely due to alcohol or sedative drug withdrawal alone; they suggest an additional focal cerebral lesion that requires evaluation.
10. Global cerebral ischemia (Chapter 13) from cardiac arrest, cardiac arrhythmias, or hypotension may produce, at onset, a few tonic or tonic–clonic movements that resemble seizures, but they probably reflect abnormal brainstem activity instead. Global ischemia may also be associated with spontaneous myoclonus (Chapter 11) or, after consciousness returns, with myoclonus precipitated by movement (action myoclonus). Partial or generalized tonic–clonic seizures also occur; these may be manifested only by subtle movements of the face or eyes and must be recognized and treated. Nonetheless, isolated seizures after global cerebral ischemia do not necessarily indicate a poor outcome.
11. Hypertensive encephalopathy (Chapter 4) may be accompanied by generalized tonic–clonic or partial seizures.
12. Eclampsia refers to the occurrence of seizures or coma in a pregnant woman with hypertension, proteinuria, and edema (preeclampsia). As in hypertensive encephalopathy in nonpregnant patients, cerebral edema, ischemia, and hemorrhage may contribute to neurologic complications. Magnesium sulfate has been widely used to treat eclamptic seizures and may be superior for this purpose to anticonvulsants such as phenytoin.
13. Hyperthermia can result from infection, exposure (heat stroke), hypothalamic lesions, or drugs such as phencyclidine, as well as anticholinergics or neuroleptics (neuroleptic malignant syndrome; Chapter 11) and inhalational anesthetics or neuromuscular blocking agents (malignant hyperthermia; Chapter 9). Clinical features of severe hyperthermia (42°C, or 107°F) include seizures, confusional states or coma, shock, and renal failure. Treatment is with antipyretics and artificial cooling to reduce body temperature immediately to 39°C (102°F) and anticonvulsants and more specific therapy (eg, antibiotics for infection, dantrolene for malignant hyperthermia) where indicated. Patients who survive may be left with ataxia as a result of the special vulnerability of cerebellar neurons to hyperthermia.
PSEUDOSEIZURES
Attacks that resemble seizures (psychogenic seizures or pseudoseizures) may be manifestations of a psychiatric disturbance such as conversion disorder, somatization disorder, factitious disorder with physical symptoms, or malingering.
Pseudoseizures usually can be distinguished both clinically and by the electroencephalogram (EEG) findings. In patients with pseudoseizures resembling tonic–clonic attacks, there may be warning and preparation before the attack; there is usually no tonic phase, and the clonic phase consists of wild thrashing movements during which the patient rarely comes to harm or is incontinent. Ictal eye closure is common. In some instances, there are abnormal movements of all extremities without loss of consciousness; in others, there is shouting, uttering of obscenities, or goal-directed behavior during apparent loss of consciousness. There is no postictal confusion or abnormal clinical signs after the attack. The EEG, if recorded during an episode, does not show organized seizure activity, and postictal slowing does not occur. The differential diagnosis should include frontal lobe seizures, which may be marked by unusual midline movements (eg, pelvic thrusting or bicycling) and by very brief postictal states. Ictal EEG abnormalities may escape detection as well.
It is important to appreciate that some patients with pseudoseizures also have genuine epileptic attacks that require anticonvulsant medications, but these should be prescribed at an empirically appropriate dose. Psychiatric referral may be helpful.
CLASSIFICATION & CLINICAL FINDINGS
CLASSIFICATION
Seizures are classified as follows:
Generalized Seizures
1. Tonic–clonic (grand mal)
2. Absence (petit mal)
3. Other types (tonic, clonic, myoclonic, atonic)
Partial Seizures
1. Simple partial
2. Complex partial (temporal lobe, psychomotor)
3. Partial seizures with secondary generalization
GENERALIZED SEIZURES
Generalized Tonic–Clonic Seizures
Generalized tonic–clonic seizures are attacks in which consciousness is lost, usually without aura or other warning. When a warning does occur, it usually consists of nonspecific symptoms.
1. Tonic phase—The initial manifestations are unconsciousness and tonic contraction of limb muscles for 10 to 30 seconds, producing first flexion and then extension, particularly of the back and neck (Figure 12-2). Tonic contraction of the muscles of respiration may produce an expiration-induced vocalization (cry or moan) and cyanosis, and contraction of masticatory muscles may cause tongue trauma. The patient falls to the ground and may be injured.
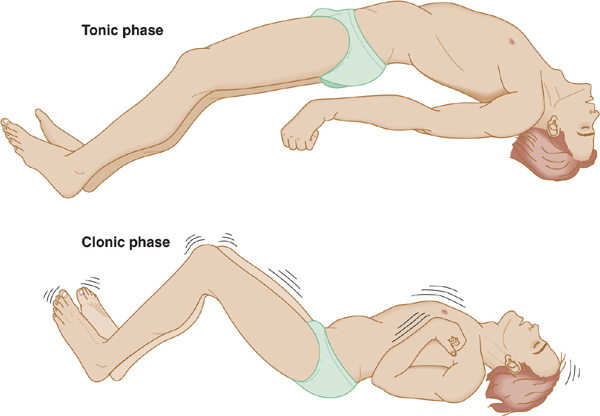
Figure 12-2. Generalized tonic–clonic seizure, illustrating the appearance of the patient in the tonic (stiffening) and clonic (shaking) phases.
2. Clonic phase—The tonic phase is followed by a clonic (alternating muscle contraction and relaxation) phase of symmetric limb jerking that persists for an additional 30 to 60 seconds or longer. Ventilatory efforts return immediately after cessation of the tonic phase, and cyanosis clears. The mouth may froth with saliva. With time, the jerking becomes less frequent, until finally all movements cease and the muscles are flaccid. Sphincteric relaxation or detrusor muscle contraction may produce urinary incontinence.
3. Recovery—As the patient regains consciousness, there is postictal confusion and often headache. Full orientation commonly takes 10 to 30 minutes or even longer in patients with status epilepticus (see next section) or preexisting structural or metabolic brain disorders. Physical examination during the postictal state is usually otherwise normal in idiopathic epilepsy or seizures of metabolic origin, except that plantar responses may be transiently extensor (Babinski sign). The pupils always react to light, even when the patient is unconscious.
4. Status epilepticus—Status epilepticus is defined arbitrarily as seizures that continue for more than 30 minutes without ceasing spontaneously or that recur so frequently that full consciousness is not restored between successive episodes. Status epilepticus is a medical emergency because it can lead to permanent brain damage from hyperpyrexia, circulatory collapse, or excitotoxic neuronal damage if untreated.
Absence (Petit Mal) Seizures
These are genetically transmitted seizures that always begin in childhood and rarely persist into adolescence. Genes linked to childhood absence epilepsy include the CACNA1H calcium channel, CLCN2 chloride channel, and GAGRB2 GABA receptor subunits. The spells are characterized by brief loss of consciousness (for 5-10 seconds) without loss of postural tone. Subtle motor manifestations, such as eye blinking or a slight head turning, are common. More complex automatic movements (automatisms) are uncommon. Full orientation immediately follows cessation of the seizure.
There may be as many as several hundred spells daily, leading to impaired school performance and social interactions, so that children may be mistakenly thought to be mentally retarded before the diagnosis of petit mal epilepsy is made. The spells are characteristically inducible by hyperventilation. The EEG shows a characteristic 3-per-second spike-and-wave pattern during the seizures (Figure 12-3). In most patients with normal intelligence and normal background activity on EEG, absence spells occur only during childhood; in other cases, however, the attacks continue into adult life, either alone or in association with other types of seizures.
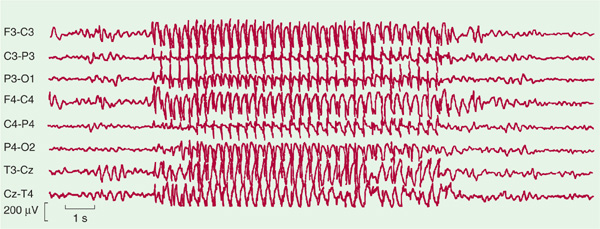
Figure 12-3. EEG of a patient with typical absence (petit mal) seizures, showing a burst of generalized 3-Hz spike-and-wave activity (center of record) that is bilaterally symmetric and bisynchronous. Odd-numbered leads indicate electrode placements over the left side of the head; even numbers, those over the right side.
Other Types of Generalized Seizures
These include tonic seizures (not followed by a clonic phase), clonic seizures (not preceded by a tonic phase), and myoclonic seizures.
1. Tonic seizures are characterized by continuous muscle contraction that can lead to fixation of the limbs and axial musculature in flexion or extension and are a cause of drop attacks; the accompanying arrest of ventilatory movements leads to cyanosis. Consciousness is lost, and there is no clonic phase to these seizures.
2. Clonic seizures are characterized by repetitive clonic jerking accompanied by loss of consciousness. There is no initial tonic component.
3. Myoclonic seizures
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


