Figure 27-1 A, Skin angiokeratoma appear as raised red lesions over the lateral flank (arrows). These are typical lesions in Fabry’s disease. B, Angiokeratomas are typically seen over pressure points, for example the knee (arrows).
Standard sensory and motor nerve conduction studies in the upper and lower extremities are normal. Sympathetic skin responses are normal in the hands but could barely be elicited in the feet. On cardiac autonomic testing, the patient had a mean R6 ratio of 1.06 (normal > 1.21), a Valsalva ratio of 1.1 (normal > 1.5), and a 30:15 ratio of 1.0 (normal > 1.04). His pulse is 96 beats per minute supine and 120/min standing, with no change in blood pressure. The cold perception threshold is >99% (insensitive) in his feet, with a normal vibration detection threshold. Extensive biochemical testing for causes of neuropathy is negative, with the exception that the α-galactosidase activity is 18% of the normal predicted value.
CONCLUSIONS
Neuropathic pain in Fabry’s disease may be chronic but typically presents with episodic crises of agonizing, incapacitating pain (Fabry’s crises) as in this patient.1 The diagnosis must be considered in younger men (incidence 1:40,000) with neuropathic pain and “small fiber” neuropathy. However, patients may present with a variety of clinical symptoms in addition to neuropathy, autonomic features, and angiokeratoma as described in this patient. Other clinical presentations include stroke (Fig. 27-2), impaired cerebellar function,2 hearing,2 left ventricular hypertrophy, renal failure, corneal whorling (Fig. 27-3) and lenticular opacities, and gastrointestinal disturbances. Nerve biopsy and dorsal root ganglion histology3 (Fig. 27-4) show the presence of Fabry’s inclusions containing glycosphingolipid globotriaosylceramide. Nerve biopsy is no longer required with the availability of measurement of enzyme levels and genetic testing. Enzyme replacement therapy may reduce pain thresholds and improve cold and heat perception in patients with neuropathic pain.2,4
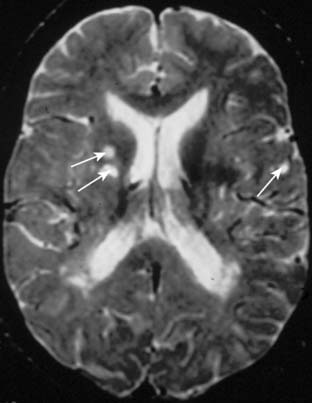
Figure 27-2 The brain magnetic resonance imaging study shows several deep subcortical lesions (arrows) including lesions in and adjacent to the internal capsule. Stroke may occur in patients with Fabry’s disease because of an associated angiopathy.
Related posts:
 Malignant Peripheral Nerve Sheath Tumor
Disseminated Sporotrichosis with Multiple Granulomatous Mononeuropathies
Late Sporadic CMT4C—A New KIAA1985 Mutation
Late-Onset Transthyretin Val30Met Familial Amyloid Polyneuropathy Unrelated to Endemic Foci
A Weak, and Numb Patient with Tremor—Antimyelin-Associated Glycoprotein Polyneuropathy
Copper Deficiency Myeloneuropathy
Malignant Peripheral Nerve Sheath Tumor
Disseminated Sporotrichosis with Multiple Granulomatous Mononeuropathies
Late Sporadic CMT4C—A New KIAA1985 Mutation
Late-Onset Transthyretin Val30Met Familial Amyloid Polyneuropathy Unrelated to Endemic Foci
A Weak, and Numb Patient with Tremor—Antimyelin-Associated Glycoprotein Polyneuropathy
Copper Deficiency Myeloneuropathy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


