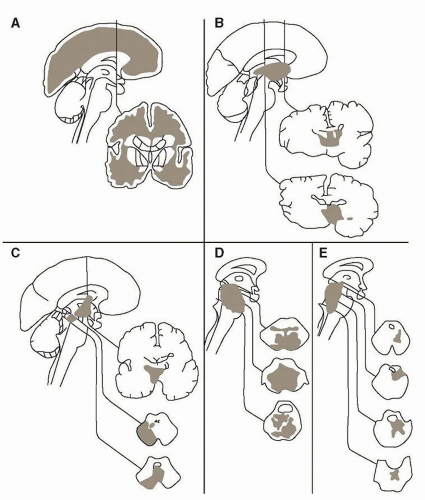
 FIGURE 18.1 Anatomy of coma. Classic brain lesions that cause coma include those located diffuse bihemispheric (A), diencephalic (B), paramedian caudal midbrain and caudal diencephalic (C), high pontine and lower midbrain paramedian tegmental regions (D), and pontine (E). (From Posner JB, Saper CB, Schiff ND, et al. Plum and Posner’s Diagnosis of Stupor and Coma. 4th ed. New York: Oxford University Press; 2007 by permission of Oxford University Press, USA.) |
TABLE 18.1 Glasgow Coma Scale | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
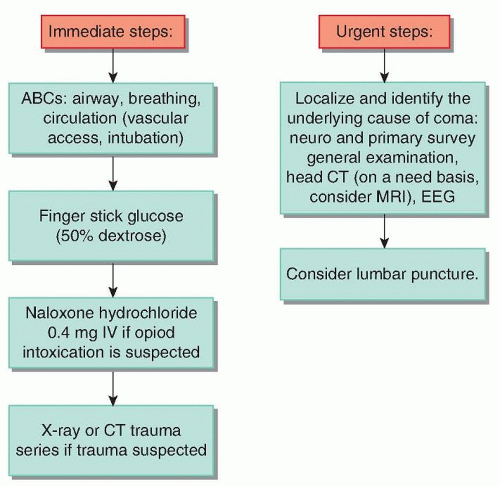 FIGURE 18.2 Management algorithm for new-onset coma. IV, intravenous; CT, computed tomography; MRI, magnetic resonance imaging; EEG, electroencephalography. |
TABLE 18.2 Practical Pearls in the Physical Examination of the Comatose Patient | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
transtentorial herniation as well (see later section for a discussion of herniation syndromes). Flexor posturing generally implies a more rostral lesion and has a better prognosis than extensor posturing, but the pattern of response may vary with different stimuli, or there may be flexion of one arm and extension of the other. When these postures seem to occur spontaneously, there may be an unrecognized stimulus (e.g., airway obstruction or bladder distention). With continuing rostrocaudal deterioration, there may be extension of the arms and flexion of the legs until, with lower brain stem destruction, there is flaccid unresponsiveness. However, lack of motor response to any stimulus should always raise the possibility of limb paralysis caused by cervical trauma, Guillain-Barré neuropathy, or the locked-in state.
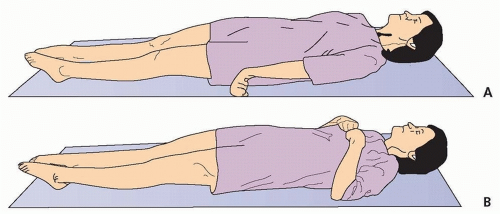 FIGURE 18.3 Decerebrate or extensor posturing (A) and decorticate or flexor posting (B). |
ping-pong gaze), may follow bilateral cerebral infarction or cerebellar hemorrhage with an intact brain stem.
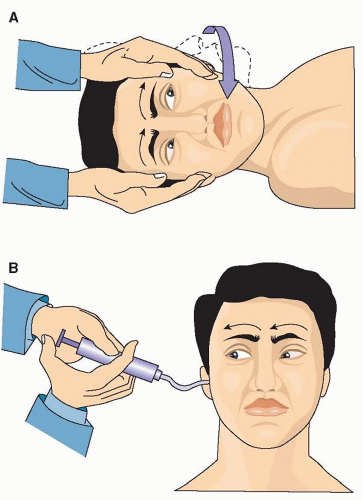 FIGURE 18.4 A: Doll’s eye maneuver (oculocephalic reflex): With intact brain stem (cranial nerves III through VIII), the eyes remain relatively stationary and move opposite to the direction of head turning. B: Cold caloric test (oculovestibular reflex): With intact brain stem, cold water in the auditory canal results in tonic conjugate eye deviation toward the cold ear. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


