Figure 62-1 Progressive, over time, recovery of sympathetic sudomotor function as documented by serial thermoregulatory sweat test representations (cartoons). The areas of the body showing normal sweating are purple, absent sweating are yellow, and untested are white. Typically in health the whole surface of the body is purple. During this patient’s recovery, the region of the surface of the body showing anhidrosis decreased from 70% to 6%.
(Reprinted with permission from Fealey RD. Thermoregulatory sweat test. In: Daube JR, Rubin DI, editors. Clinical neurophysiology. 3rd ed. New York: Oxford Univeristy Press; 2009. p. 645–60.)
Diagnosis
Testing and neurologic examination had thus confirmed the patient had a severe small fiber sensory and limited autonomic neuropathy. Combining testing done at home with ours we concluded there was evidence for a recent CMV infection just before onset of neuropathic symptoms. The evidence included initial positivity of IgM antibody to CMV that became negative months later, elevated CMV IgG during our assessment. The initial presence of splenomegaly, atypical lymphocytosis and mild hepatitis with negative EBV but positive CMV serology all supports an active CMV infection at onset. Direct invasion of the peripheral sensory and autonomic ganglia by CMV was not shown. Rather the patient was HIV negative and was immunocompetent, his serum contained ganglionic Ach receptor antibodies, and his neuropathy worsened as his CMV infection was resolving all suggesting the neuropathy was indirectly mediated by his immune response to CMV.11 This logic was behind the choice of treatment with IVIg12 instead of an antiviral agent.
Course
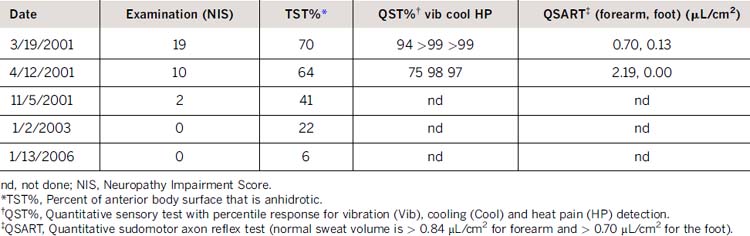
The patient was treated with one course of IVIg (0.4 g/kg/day × 7 days). Sweating and sensory function was documented via neurologic examination, TST, autonomic reflex screen and QST on his first recheck and thereafter via neurologic examination and TST. At first recheck 1 month post IVIg, the patient reported much improved dysesthesia and slight recovery of forehead and upper trunk sweating. Test results indicated minor improvement in TST (anhidrosis decreased from 70% to 64%, recovery mainly on trunk), improved forearm QSART, and slight improvement in sensation (Table 62-1). A length-dependent recovery of pain and temperature perception and sweating was noted on subsequent visits. Sensory recovery was complete after 5 years. Sweating was largely recovered after 6 years, although there was still patchy anhidrosis of the distal legs, feet, and toes on the final TST. (See Figs. 62-1 and 62-2.)
Related posts:
 Malignant Peripheral Nerve Sheath Tumor
Disseminated Sporotrichosis with Multiple Granulomatous Mononeuropathies
Late Sporadic CMT4C—A New KIAA1985 Mutation
Late-Onset Transthyretin Val30Met Familial Amyloid Polyneuropathy Unrelated to Endemic Foci
A Weak, and Numb Patient with Tremor—Antimyelin-Associated Glycoprotein Polyneuropathy
Copper Deficiency Myeloneuropathy
Malignant Peripheral Nerve Sheath Tumor
Disseminated Sporotrichosis with Multiple Granulomatous Mononeuropathies
Late Sporadic CMT4C—A New KIAA1985 Mutation
Late-Onset Transthyretin Val30Met Familial Amyloid Polyneuropathy Unrelated to Endemic Foci
A Weak, and Numb Patient with Tremor—Antimyelin-Associated Glycoprotein Polyneuropathy
Copper Deficiency Myeloneuropathy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


