Chapter 140 Surgical Management of Major Skull Defects and Potential Complications
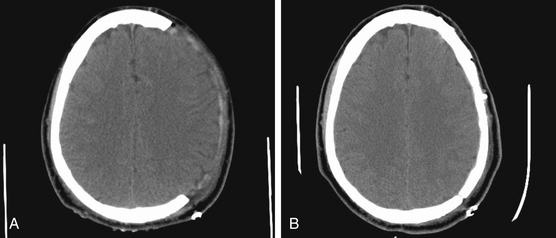
In the present era, a decompressive craniectomy is a neurosurgical procedure that describes the temporary removal of a large piece of the skull to alleviate high intracranial pressure (ICP) that can be caused by a variety of neurosurgical disorders (Fig. 140-1). In the trauma setting, two main techniques relieve high ICP: removal of the frontotemporal–parietal–occipital bone over one or both cranial hemispheres and removal of bilateral frontal bone as first described by Kjellberg and Prieto in 1971.1–3 In cases of an ischemic infarct, most craniectomies performed are removal of the frontotemporal–parietal–occipital bone over one hemisphere, and in the case of a posterior circulation infarct, a suboccipital craniectomy is generally performed. Other skull defects may result from operations in which infection or malignancies extend into the skull. The timing of the cranioplasty operation depends on the origin of the skull defect.
Historically, it has generally been recommended that cranioplasty be performed at least 3 months after initial craniectomy because this period allows sufficient time for postoperative edema to resolve and possibly reduces the rate of infection and hydrocephalus.30 However, surgeons may encounter difficulties during dissection for cranioplasty due to severe adhesion, and many surgeons advocate early cranioplasty within a month.4,5 Before the autologous bone flap can be replaced, a variety of clinical endpoints have to be established. These include a well-healed scalp with no local, systemic, or cranial infections; resolution of elevated ICP; a stable neurologic condition; and resolution of the herniation of the brain underlying the bone defect. There are several reasons reported in the literature as to why early cranioplasty helps neurologic function, one of them being the restoration of normal CSF flow dynamics.6 Communicating hydrocephalus is a common problem following a decompressive hemicraniectomy, and many authors propose early cranioplasty to prevent the requirement for permanent CSF diversion.5 Reports have revealed that CSF pressure was higher in a model with a large skull defect versus no defect,7,34 and others have shown that early cranioplasty, along with a programmable shunt, has led to reduced number of surgeries, improved patient outcomes, and reduced complications.6
In addition to hydrocephalus, the “syndrome of the trephined” is a phenomenon that improves after cranioplasty. Clinically, patients have a “sunken head” appearance on the side of the cranial defect. In 1945, Gardner described this syndrome characterized by headaches, dizziness, irritability, epilepsy, discomfort, and psychiatric symptoms occurring in patients with large cranial defects. He was the first to describe an improvement in the neurologic function of some patients undergoing cranioplasty with tantalum.8 This array of nonspecific symptoms is believed to be related to alteration of CSF dynamics, the atmosphere pressure transmitted through the unsupported scalp, and cerebral blood flow changes.9,10 Current reports characterize changes in the CSF flow dynamics, as well as increases in venous outflow.10 The sinking skin flap would transmit the atmospheric pressure to the underlying brain tissue, which would result in a low cerebral blood flow. Studies show that low cerebral blood flow increased and reached normal levels after cranioplasty.11,12
Infection following craniotomy is another situation in which the autologous bone flap is removed, and delayed cranioplasty is indicated once the infection has cleared. Reports have shown successful operative sterilization and débridement leading to avoidance of cranioplasty and preservation of the autologous bone flap.13–15 However, many situations necessitate discarding the bone flap if it has been devitalized by the infection or if the patient has an extensive scalp and brain infection. There is no clear standard time for cranioplasty after bone flap infection; intervals of 6 to 12 weeks, 6 months,16,17 and more than 12 months have been advocated.18 Assessment of the soft tissues is crucial for the timing of cranioplasty after infection. Logically, all wounds must be well healed and the scalp must be elastic enough to allow closure without excessive tension.
Bone flaps are usually placed either sterilely into a freezer or subcutaneously in the patient’s abdominal fat until time for cranioplasty. Some reports show almost identical bioactivity of the bone flap compared to the remaining intact skull and a lower reoperation rate when the bone was placed subcutaneously.19 A logical disadvantage of storing cranioplasty subcutaneously is the morbidity of an abdominal incision; alternatively, storing the flap in a freezer at −20°C or colder has been shown to be effective as a preservation method.20,21 Some reports state a large disadvantage of frozen autologous bone flap is the higher rate of resorption compared to other synthetic materials, especially in the pediatric population.22,23 Autologous bone flap infection is not uncommon; therefore, careful attention must be undertaken during storage of the flap after craniectomy. The bone flap must be cultured prior to cranioplasty; any bacterial contamination of the flap is a contraindication for reinsertion into the patient.
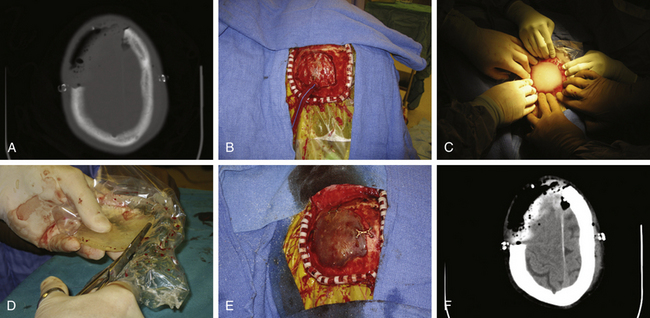
Perhaps the most common synthetic material used today is MMA (Fig. 140-2). MMA is a polymerized ester of acrylic acid that comes in a powdered form. It is relatively inexpensive when compared to other synthetic materials. When ready to use, it is mixed with a liquid monomer, benzoyl peroxide. An exothermic reaction takes place, and the MMA forms a supple substance with consistency like paste. It then cools to form a semitranslucent material that is comparable to human bone in strength. Before the final cooling process, MMA is malleable, and it can be molded to fit any skull defect. This becomes especially useful when the skull defect is a technically challenging reconstruction. This prosthesis is at a higher risk of infection than autologous bone, because it is not biologically viable and a layer of fibrous tissue grows around the allograft to which bacteria may adhere.24 Propionibacterium acnes and Staphylococcus aureus are the most common bacteria involved in postoperative craniotomy bone flap infections.25
< div class='tao-gold-member'>
Related posts:
 Cortical and Subcortical Brain Mapping
Cortical and Subcortical Brain Mapping
 Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
 Surgical Management of Tumors of the Foramen Magnum
Surgical Management of Tumors of the Foramen Magnum
 Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
 Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
 Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Arachnoid, Suprasellar, and Rathke’s Cleft Cysts



