Chapter 9 Taste and Smell
Chemical Senses
The chemical senses of taste, smell, and chemical irritation convey a range of information, warning us of environmental hazards and determining the flavor of ingested foods and liquids, whether the flavor of a food is good or bad. The pleasure experienced upon ingestion is a complex process mediated by the chemical senses (taste, smell, and irritant properties of foods) in the periphery and then multiple brain substrates, which are remarkably well conserved phylogenetically [Berridge and Kringelbach, 2008]. The degree to which the chemicals that stimulate these flavor senses are liked or disliked is determined by innate or inborn factors, learning and experience, and the interactions among these. In essence, these senses function as gatekeepers throughout the life span. They control one of the most important decisions an animal is required to make – whether to reject a foreign substance or to take it into the body, and if the substance is ingested, to inform the gastrointestinal system about the quality and quantity of the impending rush of nutrients.
The literature reviewed in this chapter suggests that human infants have functioning gustatory and olfactory systems that modulate their feeding and expressive behaviors [Ganchrow and Mennella, 2003; Mennella and Beauchamp, 2008]. Although responsiveness is evident early in development, infants are not merely miniature adults, because these chemosensory systems mature postnatally and are influenced by experiences in ways we are just beginning to understand. Because little is known about the infant’s perception of chemical irritation (e.g., sensations of burn, viscosity, and temperature resulting from stimulation of nerve endings in the soft membranes of the buccal and nasal cavities), the discussion focuses on the senses of taste and smell, but acknowledges that this other chemical sense may play an important role in the behavior of infants.
Taste, Smell, and Flavor
Taste or gustation refers to the sensation that occurs when chemicals stimulate taste receptors located on a large portion of the tongue’s dorsum and other parts of the oropharynx, such as the larynx, pharynx, and epiglottis [Doty, 2003]. The taste system is attuned to a small number of perceptual classes of experience, the so-called basic tastes, each of which specifies crucial information about nutrients or dangerous substances. These basic tastes either stimulate intake (sweet, salty, and savory) or inhibit it (bitter and perhaps sour) when ingested within a generally restricted range of concentrations.
From an evolutionary perspective, these taste qualities likely evolved to detect and reject that which is harmful and to seek out and ingest that which is beneficial. It has been hypothesized that the small number of taste qualities evolved because of the functional importance of the primary stimuli (e.g., sugars, salts, amino acids and proteins, organic acids, bitter toxins) in nutrient selection, especially during childhood. Preference for salty and sweet tastes is thought to have evolved to attract us respectively to minerals and energy-producing sugars and vitamins. Rejection of bitter-tasting and irritating substances evolved to protect the animal from being poisoned and the plant producing these chemicals from being eaten [Jacobs et al., 1978; Glendinning, 1994]. This rejection is commonly observed when children reject the bitter taste of green vegetables or many liquid formulations of drugs. Rejecting the bitter taste of medicine can, however, thwart the benefits of even the most powerful drugs. Many active pharmaceutical ingredients taste bitter or irritate the mouth and throat. Effective methods of avoiding unpleasant tastes for adults, encapsulating the medicine in pill or tablet form, are problematic since many children cannot or will not swallow either preparation. However, while bitter tastes are innately disliked, with experience people may come to like certain foods that are bitter, particularly some vegetables, and foods and beverages with pharmacologically active bitter compounds, such as caffeine or ethanol.
By being intimately connected to the ingestion or rejection of foods via hedonics, taste and olfaction can contribute to weight loss or gain, and when healthful foods are avoided, can pose a nutritional risk [Mattes and Cowart 1994; Doty, 2009]. Further, excessive intake of foods containing highly preferred tastes (sweet, salty) because of their strong hedonic component may cause or exacerbate a number of illnesses, including hypertension and diabetes. Beyond nutrition, sweet taste is linked to brain pathways involved in reward processing and learning. Many drugs of abuse, which give pleasure, exert their influence through some of these same pathways, and consequently there are many biological commonalities between overconsumption of sweets and drug addiction [Pepino and Mennella 2007; Berridge and Kringelbach 2008; Levine et al., 2003].
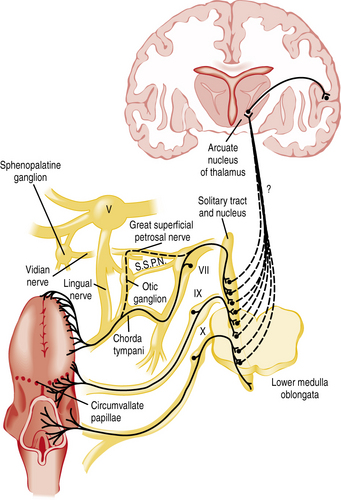
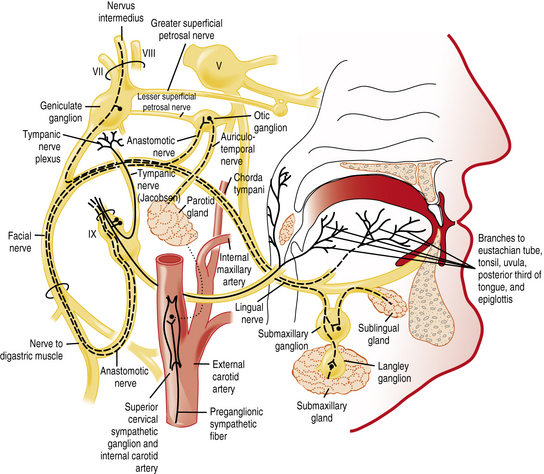
The chemicals that elicit taste qualities are detected not only by specialized receptors on the tongue and other parts of the oral cavity, but by the gastrointestinal system as well [Egan and Margolskee, 2008]. The taste receptors in the oral cavity are localized in taste buds and are innervated by branches of three cranial nerves: the facial (VII), glossopharyngeal (IX), and vagal (X) nerves (Figure 9-1 and Figure 9-2). During the past decade, major progress has been made in identifying the initial events in taste recognition [Bachmanov and Beauchamp, 2007; Chandrashekar et al., 2006; Katz et al., 2008; Kim et al., 2006]. It appears that two different strategies have evolved to detect taste molecules. For salty and sour tastes, it is widely believed that ion channels serve as receptors. Here H+ (sour) and Na+ (salty) ions are thought to flow through the channels into the cell. The cell is then activated and sends an electrical message to the brain. However, for both of these taste qualities, the molecular identity of the receptors and their exact mechanisms are still unknown. For sweet, umami, and bitter tastes, G-protein coupled receptors (GPCRs) appear to play the most prominent roles. These GPCRs bind taste molecules in a sort of lock-and-key mechanism, thereby activating the taste cell to send an electrical message to the brain. For sweet and umami, a family of three GPCRs, named T1R1, T1R2, and T1R3, act in pairs (T1R1+T1R3 for umami, and T1R2+T1R3 for sweet) to detect molecules imparting these taste qualities. A substantially larger family of GPCRs, the T2Rs (around 25), constitutes the bitter receptors.
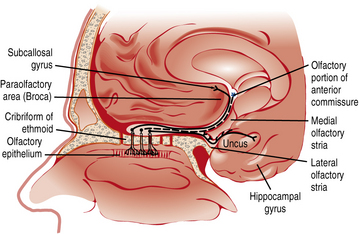
Smell or olfaction occurs when chemicals stimulate olfactory receptors located on a relatively small patch of tissue high in the nasal cavity (Figure 9-3) [Doty, 2003, 2009]. The organization of the olfactory system reflects the need to recognize a wide range of odors and to discriminate one odor from another. There are several noteworthy differences between the taste and smell system. First, unlike the gustatory receptors, the olfactory neurons are the actual receptor cells and are uniquely exposed to the external environment. Second, they can regenerate from basal cells after being damaged. Third, the olfactory receptors are served by only a single cranial nerve (I). Fourth, there is a much larger number of odor qualities, as suggested by the identification of a large family of genes that apparently code for a large number of receptor proteins located on membranes of the cilia of olfactory neurons [Buck and Axel, 1991]. In fact, the olfactory receptor genes are encoded by the largest mammalian gene superfamily of more than 1000 genes [Buck and Axel, 1991]; however, more than half of this receptor gene family are pseudogenes in humans [Gilad et al., 2003]. Fifth, odor stimuli can reach the olfactory receptors in two ways. Odor molecules can reach the olfactory receptors by entering the nostrils during inhalation (orthonasal route) or by travelling from the back of the oral cavity toward the roof of the nasal pharynx (retronasal route). It is this retronasal stimulation arising from the molecules of foodstuffs that leads to many of the flavor sensations we experience during eating.
Although there is some evidence that some odors may be innately biased in a positive or negative direction [Khan et al., 2007], individual experiences largely determine how much a person likes or dislikes the odor component of a food or beverage flavor. Through experiences, odors acquire personal significance [Forestell and Mennella, 2005; Mennella and Forestell, 2008; Mennella and Garcia, 2000]. Memories evoked by odors are more emotionally charged and resistant to change than those evoked by other sensory stimuli [Herz and Cupchik, 1995]. The unique processing of olfactory information [Cahill et al., 1995], and the olfactory system’s immediate access to the neurological substrates underlying nonverbal aspects of emotion and memory [Royet and Plailly, 2004], help explain the large emotional component of food aromas. This, coupled with the recent finding that the most salient memories formed during the first decade of life will likely be olfactory in nature [Willander and Larsson, 2006], explains how food aromas can trigger memories of childhood and why flavors and food aromas experienced during childhood remain preferred, and to some extent, can provide comfort.
Flavor, as an attribute of foods and beverages, is defined as the integration of multiple sensory inputs of the taste, retronasal olfaction, and irritation of a substance in the oral and nasal cavities. However, the perceptions arising from the taste and smell senses are often confused and misappropriated [Rozin, 1982], with sensations such as vanilla, fish, chocolate, and coffee being erroneously attributed only to the taste system, although much of the sensory input results from retronasal olfaction. Holding the nose while eating interrupts retronasal olfaction and thereby eliminates many of the subtleties of food or medicines, leaving the taste components remaining. Another example of the importance of olfaction in flavor perception is the inability to discriminate common foods when olfactory receptors are blocked by an upper respiratory infection.
Clinical Disorders of Taste and Smell
The common confusion between taste and retronasal olfaction is highlighted because many patients, young and old, report they cannot taste when they suffer only from olfactory loss [Cowart et al., 1997; Pribitkin et al., 2003]. The sense of smell appears to be more vulnerable than that of taste, in part because of the differences described earlier. Approximately two-thirds of patients who present to specialized chemosensory clinics complained of taste loss, but most patients were diagnosed with a measurable smell rather than gustatory dysfunction, as the basis of their “taste” complaint [Cowart et al., 1997]. A retrospective review of the 1176 patients evaluated for chemosensory dysfunction complaints at the Monell–Jefferson Chemosensory Clinical Research Center in Philadelphia revealed that severe, generalized taste deficits (i.e., complete or nearly complete taste loss) do occur but are extremely rare (<1 percent of patients), whereas profound olfactory deficits are more common (32 percent of patients) [Pribitkin et al., 2003]. A complete listing of the taste and smell centers that specialize in the assessment and treatment of chemosensory problems, along with information about the National Institute on Deafness and Other Communication Disorders (NIDCD) clearinghouse, a national resource center for information about hearing, balance, smell, taste, voice, speech, and language for health professionals, patients, industry, and the public, can be found in Box 9-1.
Box 9-1 Clinics Specializing in Disorders of Taste and Smell
University of Florida McKnight Brain Institute’s Center for Smell and Taste
100 S Newell Drive, Room L1-100J
* Indicates centers that are supported by the National Institute on Deafness and Other Communication Disorders (NIDCD), one of the National Institutes of Health. The NIDCD supports and conducts research and research training on the normal and disordered processes of hearing, balance, smell, taste, voice, speech, and language, and provides health information, based upon scientific discovery, to the public. The NIDCD Information Clearinghouse can be reached by calling (800) 241-1044 (voice) or (800) 241-1055 (TTY), 8:30 am to 5:00 pm (ET), or by sending an e-mail to nidcdinfo@nidcd.nih.gov. For more information about NIDCD programs, visit the website at www.nidcd.nih.gov.
Although complete taste loss is rare, clinical disorders that influence taste and smell perception are more common. The confusion between taste and retronasal olfaction underscores the need for careful sensory evaluation of these causes and helps explain why patients’ description of the complaint are often inaccurate. Moreover, clinical disorders that influence taste perception involve multiple organ systems and require a multidisciplinary approach for appropriate diagnosis and management [Bromley and Doty, 2003; Hoffman et al., 2009]. Particular attention should be paid to the history of problems with speech articulation, salivation, chewing, swallowing, oral pain or burn, otitis media, mouth dryness, periodontal disease, foul breath odor, recent dental procedures and surgeries, recent radiation exposure, medications, bruxism, and dietary changes. Questions about hearing, tinnitus, and balance may reveal useful information because the vestibulocochlear nerve travels near the facial nerve and is susceptible to similar conditions [Bromley and Doty, 2003].
The neurologic examination should pay particular attention to the first (olfactory), fifth (trigeminal), seventh (facial), ninth (glossopharyngeal), and tenth (vagus) cranial nerves and their central connections. Frontal lobe function and signs of increased intracranial pressure, such as papilledema and abducens nerve palsies, should be assessed [Barwick, 1989]. The oral cavity should be checked for dryness, inflammation, infections, and suspicious lesions. The tongue should be palpated to detect masses, neoplastic lesions, or collections in the tongue’s musculature, and its color, presence of plaque, and degree of salivation should be evaluated. Of particular importance are the appearance of teeth, gums, and taste papillae, and the color of the dorsal surface of the tongue (i.e., white, brown, or red [atrophic]) [Spielman, 1998]. For some gustatory disorders, a detailed dental history may be helpful. The nasal cavity and sinuses should be checked because the color of the mucosa, presence of a purulent discharge, edema, and atrophy may indicate a condition that can affect olfactory functioning [Snow et al., 1991]. Newer endoscopes (e.g., Storz) may assist in visualizing the olfactory epithelium. Sinus radiographs may be useful when evaluating ethmoid or diffuse sinus disease, whereas computed tomographic (CT) scans may be indicated if intracranial or sinus disease is suspected. However, no significant relation has been found between the size of the nasal and sinus structures as assessed by CT scans and smell ability in adults [Hong et al., 1998]. Magnetic resonance imaging (MRI), the method of choice for soft-tissue anatomy and central nervous system (CNS) structures, has been used to evaluate sites of injury in patients with post-traumatic olfactory deficits [Yousem et al., 1996]. MRI of the oropharynx and neck should be conducted for patients presenting with ageusia (complete loss of taste), to exclude hematoma or abscess of the tongue and surrounding tissues [Pribitkin et al., 2003]. Gustatory dysfunction has been related to MRI-established ischemia, hemorrhage, or demyelination plaques in the brainstem and higher cortical areas in some patients with chronic dysgeusia [Bromley and Doty, 2003].
In addition to a careful medical history and otolaryngologic examination, assessment of a smell or taste complaint should involve standardized testing using a variety of psychophysical techniques (e.g., detection thresholds, magnitude estimates, quality identification) in a clinical setting [Cowart et al., 1997; Frank et al., 2003; Pribitkin et al., 2003; Snyder et al., 2006]. For example, patients are often asked to identify the taste quality (i.e., sweet, sour, bitter, salty) of a solution that is sipped or to identify an odor that is smelled. Retronasal olfactory function also should be assessed [Heilmann et al., 2002; Pierce and Halpern, 1996]. For younger pediatric populations, age-appropriate odorants (i.e., baby powder, bubble gum, candy cane, licorice, and peach) are recommended [Richman et al., 1995]. A commercially available scratch-and-smell test, the University of Pennsylvania Smell Identification Test (Sensonics, Inc., Haddon Heights, NJ; www.sensonics.com), has found widespread acceptance because of its relative ease of administration. In addition to identification, detection thresholds and intensity functions can be determined by having patients signify, usually verbally, the presence, absence, or intensity of a taste or smell stimulus presented at various concentrations [Bartoshuk et al., 1987; Frank et al., 2003].
The lack of standardized methodology and the need for testing methods suitable for clinical and field assessment [Snyder and Bartoshuk, 2009; Hoffman et al., 2009] is magnified when the clinician or researcher needs to evaluate olfactory and taste functioning in young children. First, because young children are more prone to attention lapses and have shorter memory spans, any method relying on sustained attention that places demands on memory could yield spurious findings. Second, because young children tend to answer questions in the affirmative, a forced-choice categorization procedure is generally preferred. Age-appropriate tasks, embedded in the context of a game that is fun for children and minimizes the impact of language and cognitive development, are particularly effective [Schmidt and Beauchamp, 1988; Forestell and Mennella, 2005; Mennella et al., 2005, 2011]. Third, children are likely to be unfamiliar with many of the odor stimuli used in adult tests and have limited ability to read and identify labels to select from alternative choices, which is the typical adult response option [Dalton et al., 2009]. To address this gap in appropriate methodology, the National Institutes of Health (NIH) Blueprint for Neuroscience Research was established and then funded the Toolbox Initiative (see www.nihtoolbox.org) to assemble brief, comprehensive assessment tools that can be used by clinicians and researchers in a variety of settings in four domains: cognition, emotion, sensation, and motor. Included in sensation domain is the development and validation of a specialized battery of tests to assess both taste [Mennella et al., 2011] and smell sensitivity (the analytic precision of the sensory system) and hedonics (pleasantness, liking, or preference) for diverse populations from 3 to 85 years of age (visit www.nihtoolbox.org for updates).
As shown in Box 9-2 and Box 9-3, disorders of taste and smell in adults (and presumably in younger patients) can arise from a variety of sources, including medications, radiation therapy, nutritional deficiencies, metabolic changes, head trauma, otitis media, tonsillectomy, chronic disorders of the nasal epithelia, neurologic disorders such as tumors, viral infections, endocrine imbalances, aging, and environmental exposure [Cowart et al., 1997; Doty, 2003, 2009; Doty et al., 2003; Mott and Leopold, 1991; Murphy et al., 2003; Schiffman, 1983; Spielman, 1998]. However, many of the conditions listed are based on adult patients’ reports and not on standardized test assessments of chemosensory functioning or controlled clinical trials.
Box 9-2 Conditions Associated with Disturbances of Taste
























































(Data from Mott AE, Leopold DA. Disorders in taste and smell. Med Clin North Am 1991;75:1321 and from Bromley SM, Dory RL. Clinical disorders affecting taste: Evaluation and management. In: Dory RL, ed. Handbook of olfaction and gustation, 2nd edn. New York: Marcel Dekker, 2003:935.)
Box 9-3 Conditions Associated with Disturbances of Olfaction























































(Adapted from Mott AE, Leopold DA. Disorders in taste and smell. Med Clin North Am 1991;75:1321.)
Despite advances in our understanding of the mechanisms and functions of the chemical senses, there are no internationally accepted standards of impairment for the chemical senses [Hoffman et al., 2009], and the treatment options for taste and smell disorders remain limited. Olfactory dysfunctions resulting from impairment of odor access to the olfactory receptors may be treated. For example, patients may experience improvements in olfactory ability after adenoidectomy [Ghorbanian et al., 1983] or surgical management of nasal polyps because of the re-establishment of nasal airflow [but see Doty and Mishra, 2001]. However, those individuals whose source of deficit lies within the olfactory neuroepithelium or central olfactory or cortical pathways typically have no treatment options available other than time and possible spontaneous recovery. Similarly, the prognosis for severe taste loss is mixed, and delayed, gradual recovery was the most common pattern observed in such patients [Pribitkin et al., 2003]. Although zinc supplementation has received considerable attention as a treatment for taste loss, two double-blind studies failed to determine a benefit compared with placebo [Henkin et al., 1976; Yoshida et al., 1991].
The Ontogeny of Taste Perception and Preferences
Fetus and Preterm Infants
Although amniotic fluid and embryonic membranes provide a series of barriers that protect the fetus from outside world disturbances, the fetus is nevertheless exposed to a variety of chemosensory stimuli in utero. The composition of amniotic fluid varies over the course of gestation, particularly as the fetus begins to urinate, so that by term, the human fetus is actively swallowing almost a liter per day and has been exposed to a variety of substances, including glucose, fructose, lactic acid, pyruvic acid, fatty acids, phospholipids, creatinine, urea, uric acid, amino acids, proteins, and salts [Liley, 1972].
The taste system is well developed before birth. The apparatus needed to detect taste stimuli, the taste buds, makes its first appearance around 7 or 8 weeks’ gestation, and by 13–15 weeks, the taste bud begins to resemble the adult bud morphologically, except for the cornification overlying the papilla [Bradley, 1972]. Taste pores, which provide the access for taste stimuli to interact with taste receptor cells, are present in fetal fungiform papillae before the end of the fourth month [Bradley, 1972; Hersch and Ganchrow, 1980; Witt and Reutter, 1997]. There is some evidence, albeit weak and indirect, for preferential responding to taste stimuli in the human fetus. Clinical observations of differential fetal swallowing after the injection of sweet or bitter substances into the amniotic fluid suggest that the fetus prefers sweet and rejects bitter, but these observations are inconclusive because of the methodologic limitations in measuring fetal responses [DeSnoo, 1937; Liley, 1972].
Another approach used in determining whether taste perception and preferences are present before birth is to study preterm infants. Such studies reported increased salivation in response to oral presentations of a drop of pure lemon juice, diminished suckling in response to quinine solutions, and enhanced suckling in response to glucose compared with water [Tatzer et al., 1985]. Because premature infants are at risk for aspirating fluids because of immature suck–swallow coordination, a method was developed that did not necessitate the delivery of any fluids while administering a taste. The taste substance was embedded in a nipple-shaped gelatin medium that released small amounts of the substance when it was mouthed or sucked. Infants, born preterm and tested between 33 and 40 weeks after conception, produced more frequent, stronger sucking responses when offered a sucrose-sweetened nipple compared with a nonsweet latex nipple [Maone et al., 1990].
In conclusion, studies on premature infants support the hypothesis that preference for sweet taste is evidenced before birth. These data also suggest that taste buds are capable of conveying gustatory information to the CNS by the third trimester of pregnancy, and this information is available to systems organizing changes in sucking, facial expressions, and other affective behaviors [Ganchrow and Mennella, 2003].
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


