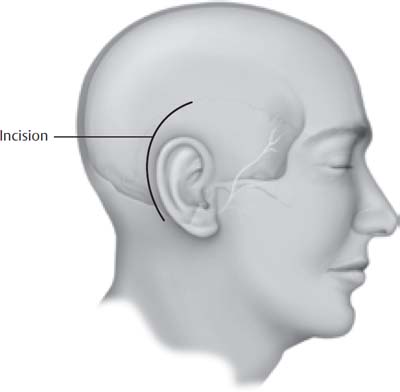
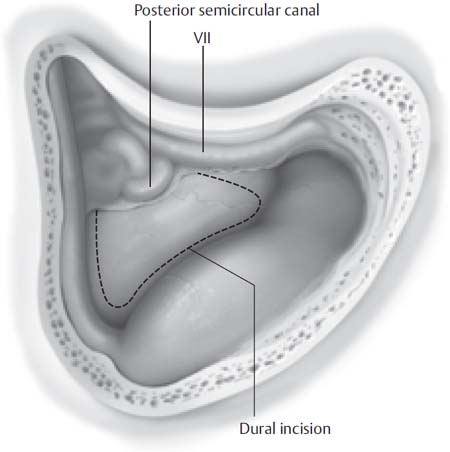
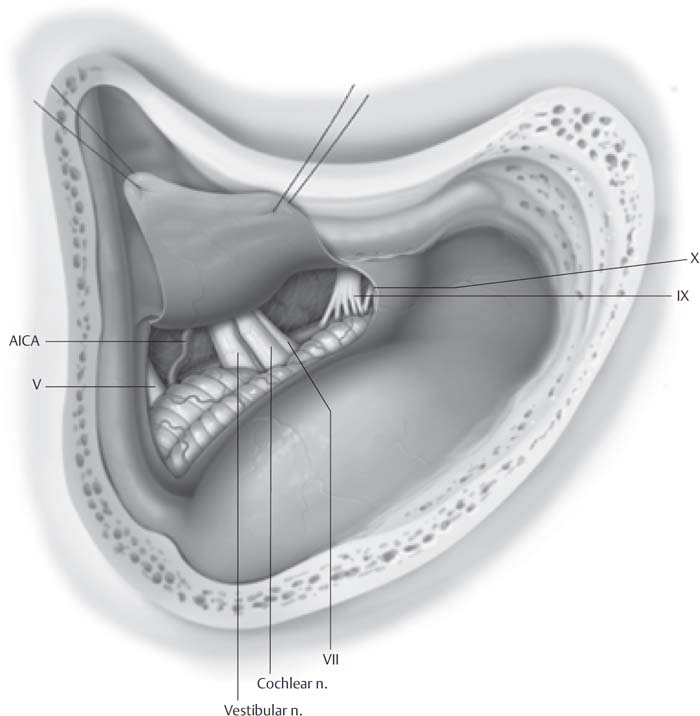
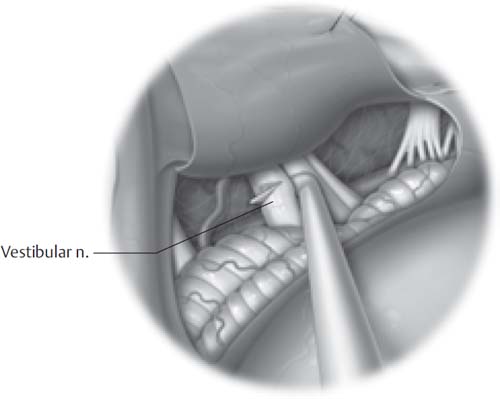
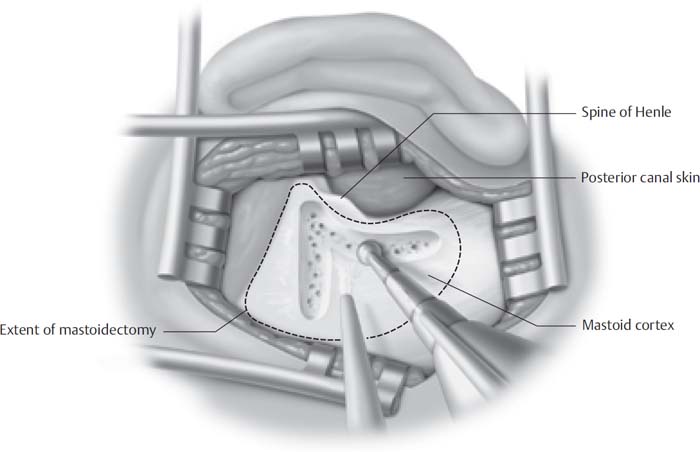
17 This final chapter enumerates the surgical techniques that we have developed to facilitate operative exposure, preservation of the facial nerve, preservation of the cochlear nerve, and avoidance of injury to adjacent neurologic structures, such as the brainstem and regional cranial nerves. We discuss the following operations: the suboccipital retrolabyrinthine craniotomy with vestibular nerve section, the middle fossa craniotomy, and the suboccipital translabyrinthine craniotomy. The indications for this procedure are refractory Meniere’s disease or other pathology involving the vestibular nerves. It can be performed in association with an endolymphatic shunting procedure. The procedure is performed with the patient in a supine position with the head turned away from the involved side. Head tongs are not necessary. If the neck is stiff and the degree of rotation is limited, the operating table itself can be rotated to compensate. The skin incision should be at least a fingerbreadth behind and parallel to the helix of the involved ear (Fig. 17.1). If the incision is too far forward in the auricular crease, the necessary bony dissection beneath the skin will be virtually impossible. One of the key considerations in this operation, and in fact all operations through the temporal bone, is adequate exposure—the sine qua non of all temporal bone surgery. The skin is reflected and held in place with retractors exposing the underlying mastoid and subocciput. A complete mastoidectomy is then performed. Bones should be completely removed over the sigmoid sinus so it can be easily decompressed. At least a centimeter of bone should be removed from the suboccipital area posterior to the sinus (Fig. 17.2). This is as critical (if not more so) than for the suboccipital translabyrinthine approach. If this is not done completely, a bothersome bony ridge will prevent adequate exposure in the cerebellopontine angle after the dura has been opened. Bone should be removed over the dura overlying the temporal lobe. It is far better and safer to make sure the bony exposure is adequate before opening the dura. To complete the bony dissection, bone should be removed medial to the posterior semicircular canal as far anteriorly as possible (Fig. 17.2). If the posterior semicircular canal is laterally placed, dissection can be performed almost to the internal auditory canal. One of the errors in the performance of this operation is inadequate bone removal. The importance of bone removal as described above cannot be overemphasized. If it is done properly, the procedure flows smoothly. If it is inadequate, it is impossible to clearly delineate cranial nerve VIII in the cerebellopontine angle. Fig. 17.1 Postauricular incision. The dural opening is squarely shaped with one limb inferior to the superior petrosal sinus and the other limb anterior to the sigmoid sinus (Fig. 17.3). The underlying cerebellum relaxes after removal of spinal fluid from the cisterna lateralis. Gentle pressure on the cerebellum using only a suction tip, with or without a cottonoid strip, will usually suffice to open the cistern. Once the cerebellopontine angle has been exposed, it is important to recognize the position and the relationships of cranial nerves VII and VIII. Occasionally they will be obscured by a small lobe of cerebellum. The cerebellum can sometimes be herniated into the porus of the internal auditory canal. This lobe of cerebellum should be carefully dissected free from the internal auditory canal. Then the plane between the cerebellum and the nerves can be cleanly developed. Fig. 17.2 Retrolabyrinthine posterior fossa and sigmoid sinus decompression. Fig. 17.3 The dura is opened and the cochleovestibular/facial nerve complex is exposed. AICA, anterior inferior cerebellar artery. The vestibular division of the cochlear nerve lies superior to the cochlear division in the cerebellopontine angle (Fig. 17.3). This is because of the rotation of cranial nerve VIII that occurs after it exits the internal auditory canal. The facial nerve usually lies anterior to cranial nerve VIII but occasionally will be superiorly placed, being very close to the vestibular division. It is extremely important to ascertain the position of the facial nerve with the facial nerve monitor. A small sharp hook can then be used to separate the fibers of the vestibular division from the cochlear division. This dissection is done on the superior aspect of cranial nerve VIII in an anterior to posterior direction. This method of dissection is utilized because of the kidney-bean shape of cranial nerve VIII in cross section. A glistening plane is usually visible between the vestibular and cochlear divisions when the section is complete (Fig. 17.4). Fig. 17.4 Using a hook, the vestibular nerve is separated from the cochlear nerve and cut. After completion of the section, the dura is sutured. The cavity is filled with abdominal fat and then covered with titanium mesh, which is fixed to the underlying bone with metallic screws. The suboccipital translabyrinthine craniotomy is an extension of the suboccipital retrolabyrinthine craniotomy as described above. The additional dissection in this operation entails a complete labyrinthectomy, exposure of the internal auditory canal, and the labyrinthine portion of the facial nerve. This will assist in the retraction necessary for the further exposure needed in this procedure (Figs. 17.5, 17.6, 17.7, and 17.8). The dura is opened over the posterior fossa and the internal auditory canal (Fig. 17.9). The cut dural edges are tented up superiorly and inferiorly using 4-0 suture. In the situation where there is a large underlying tumor, it is extremely important to decompress the cisterna lateralis of spinal fluid. This can be done either by retraction of the cerebellum using cottonoid strips and a suction device or removal of a portion of the interior of the tumor. These maneuvers usually open up the cisterna lateralis and release the spinal fluid. After this has been accomplished, the intracranial pressure will be relaxed and exposure in the cerebellopontine angle will be facilitated. If the tumor is small, facial nerve dissection starts at the end of the internal auditory canal. Previously the labyrinthine portion of the facial nerve has been identified (Fig. 17.10). Starting from this known identifiable position at the lateral extent of the internal auditory canal, facial nerve dissection can begin. Cranial nerve VIII is cut laterally and all tumor is removed from the fundus of the internal auditory canal. The establishment of a plane between the facial nerve and the tumor at the lateral extent of the internal auditory canal is extremely important. The dissection in this plane can be developed down to the origin of the facial nerve at the brainstem. This in effect facilitates the total removal of the tumor. Care must be taken to avoid stretching of the facial nerve with small tumors that have not been already stretched over time with tumor growth. This is critical. The dissection of a large tumor is of course much more difficult. The course of the facial nerve over the dome of the tumor is variable and must be considered. The dissections of tumors with an anteriorly placed facial nerve are in general less complicated than for a superiorly placed facial nerve. The exact position of the facial nerve should be ascertained early in the procedure. Before the facial nerve can be saved and dissected free, the main mass of the tumor must be debulked and delivered. In our hands this can be accomplished either with the ultrasonic aspirator or the Urban rotary dissector. The tumor is usually crushed over small areas with a cupped forceps to allow better uptake with either of these instruments. Once the main mass of the tumor has been removed, the point of origin of the facial nerve from the brainstem can be ascertained. Having the lateral and medial portions of the facial nerve delineated facilitates the final delivery of the nerve from the tumor. Dissection of the facial nerve from the tumor is performed with sharp dissection, avoiding tension or pulling on the facial nerve as much as possible. This part of the dissection can be extremely difficult. Occasionally a small scrap of tumor may be left on the facial nerve if it is apparent that removing it will result in loss of continuity of the nerve. Fig. 17.5 Cortical mastoidectomy.
The Fine Points of Posterior Fossa Surgery
 The Suboccipital Retrolabyrinthine Craniotomy with Vestibular Nerve Section
The Suboccipital Retrolabyrinthine Craniotomy with Vestibular Nerve Section
 Suboccipital Translabyrinthine Craniotomy
Suboccipital Translabyrinthine Craniotomy
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The Fine Points of Posterior Fossa Surgery
