balance may be less than pristine especially with advancing age. Slight asymmetries, particularly in the face, are commonly found during neurologic examination in normal individuals and likely do not hold much clinical relevance. Some reviews have suggested that soft neurologic signs including poor motor coordination, sensory perception, and motor sequencing may occur in as much as half of all healthy individuals. Understanding when to strongly consider finding, simply record it, or to discard it altogether often takes a very skilled examiner cautiously interpreting each finding. However, this need not take a fully refined neurologist to make such decisions, particularly if one approaches the neurologic examination with a clear sense of the likely localization as suggested by a fully developed history. When findings are found in isolation, particularly without a clear connection to the history that has just been developed, it may be justifiable to recognize and record the finding but not necessarily dwell on it. A neurologist typically will take these findings into consideration and tailor, repeat, or perform additional elements of the neurologic examination to assure that the finding is simply an isolated finding (and perhaps even a normal variation) or a relevant new finding. In addition, it is certainly acceptable upon discovery of a subtle neurologic finding to reask a newly relevant history, which may not have otherwise been apparent despite a seemingly comprehensive initial history.
TABLE 3.1 The Neurologic Exam | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
standardized cognitive screening examination will often have been developed in the context of hundreds, if not thousands, of applications and multiple social economic and cultural contexts, making its interpretation more generalizable. Second, at the level of the examiner, use of the same examination repeatedly may give the examiner greater confidence in examination skill and interpretation based on a learned experience of typical or expected responses developed over the course of giving the same test in multiple clinical contexts. Third, most standardized mental status examinations allow for a hierarchical approach to understanding someone’s cognitive abilities. For instance, for a task of delayed recall, it is important to understand not only what a patient can freely recall but also what the patient may recognize either through the contextual or categorical clue given for recognition tasks or subsequently through list of forced choices. Using a sequential, hierarchical approach to assessing memory abilities allows for determination of free word retrieval (presumably a harder response) versus recognition (by choices), which are thought to be independent of registration tasks. Finally, serial assessments of an individual patient may require adjustment of exam techniques to avoid the potential effects of learning or practice.
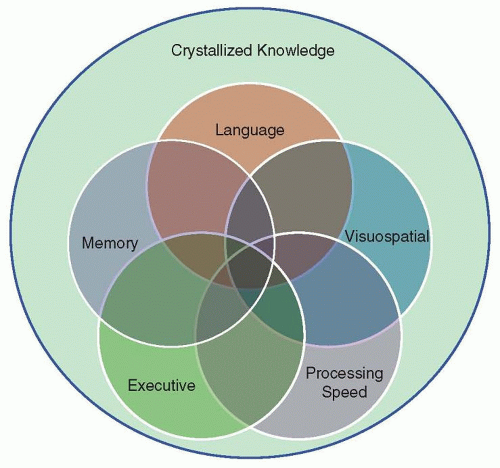 FIGURE 3.1 Conceptual framework for the mental status examination and interpretation. Each of the five principal cognitive domains (language, memory, visuospatial, processing speed, and executive function) are drawn from a series of tests comprising the mental status examination. Relative strengths and weaknesses in each domain may be inferred based on a series of related tests which map potentially to several domains but relatively consistently identify a domain of impairment. The interpretation of each abnormality must be considered within the context of each test, including normative information if known. The relative function of each domain is likely influenced by and superimposed on crystallized knowledge, which conceptually summarizes education, life experiences, and cognitive reserve. |
presentations, and may have differing meanings depending on the person reviewing the examination described by others. A formal description of various forms of memory is provided in summary in Table 30.2. Working memory is generally considered to be the online or in-the-moment memory, such as what may be used when repeating a series of unrelated words or number sequence. Short-term memory involves testing a set of ideas registered with the patient and specifically queried by the examiner after a delay of several minutes. Items not freely recalled but instead recognized from a list (recognition) can be additionally informative. Long-term memory can either represent a more prolonged delay in testing responses to the task of recollection, or in some other tasks may instead represent long-term general or autobiographical knowledge. It is important to document the content asked to be remembered and the duration of time until asking for retrieval of information. Recall is entirely predicated on the patient’s ability to register several items to be recalled, and this begins with preparing patient for this task in a minimally distracting environment.
low-frequency relative to high-frequency words, as is often seen in disorders like Alzheimer disease. In addition, the naming examination may be tailored to the patient for objects well-known in the context of their life experience or profession, such as images of a set of carpenter’s tools. A number of forms of specific categorical dysnomic aphasias are known to exist, such as color dysnomia, and should be tested in the appropriate clinical context.
TABLE 3.2 Types of Aphasia Types of Aphasia | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


