CHAPTER 223 Thoracolumbar Spinal Disorders in Pediatric Patients*
Disorders of the pediatric thoracolumbar spine include a remarkably diverse range of conditions arising from congenital, developmental, and acquired pathologies (Table 223-1). In distinct contrast to adult spinal disorders, pediatric spinal disorders are not typically related to the degenerative aging process. Parallel contrasts in the management of pediatric and adult spinal disorders also exist, not only because of the differing common pathologies but also because of the growth potential of the immature spine and the long-term functional expectations. Effective care of pediatric patients with spinal disorders requires an understanding of the pathologies encountered, the means by which these patients are clinically evaluated, and the strategies, both nonoperative and operative, by which these patients are managed. Toward this end, this chapter provides a basic overview of thoracolumbar spinal disorders of the pediatric spine.
TABLE 223-1 Causes of Pediatric Thoracolumbar Spinal Disorders
Modified from Smith JS, Abel MF, Shaffrey CI, et al. Decision making in pediatric spinal deformity. Neurosurgery. 2008;63(3 suppl):54-68.
Clinical Evaluation of Pediatric Spine Patients
Initial evaluation of a pediatric patient with a suspected spinal condition should begin with a complete history, including the prenatal and birth history, as well as the cognitive and motor developmental history.1 Details with regard to the suspected spinal disorder should be documented, including symptoms, deficits, and the time course over which they have developed and progressed. In addition, attention should be directed to the degree to which the symptoms, deficits, and deformity have had an impact on the ability to function and the quality of life of the patient. The past medical history and current medical concerns should be carefully reviewed because it is not uncommon for pediatric spinal disorders, especially congenital spinal disorders, to be accompanied by other anomalies that may warrant further investigation. For example, anatomic and physiologic abnormalities of the renal, respiratory, and cardiac systems may be associated with congenital spinal disorders.2
Imaging Evaluation of Pediatric Spine Patients
Imaging studies are invaluable in the evaluation of spinal disorders, and selection of the appropriate studies should be guided by the patient’s history and physical examination, as well as by the suspected pathology. Initial evaluation of a patient with a suspected spinal deformity often includes full-length (36-inch) posteroanterior (PA) and lateral spine radiographs to provide assessment of global and regional spinal alignment. For patients able to stand, these radiographs should be obtained in a standing position, and care should be taken to ensure that the legs are straight, specifically that the knees are not bent and the hips are not flexed. PA images may be used to assess for scoliosis, with measures including Cobb’s angle and coronal balance. Coronal balance is typically measured as the distance between a line dropped vertically from the center of the C7 vertebral body (C7 plumb line) and the central sacral vertical line (CSVL) (Fig. 223-1A). With the PA image in a true-left/true-right orientation, displacements of the C7 plumb line to the left of the CSVL are reflected as negative values, and displacements to the right of the CSVL are reflected as positive values. Lateral full-length spinal radiographs can be used to assess for regional kyphosis and lordosis and for global sagittal balance. Sagittal balance is typically measured as the distance between a line dropped vertically from the center of the C7 vertebral body (C7 plumb line) and the posterior superior corner of the S1 vertebral body (Fig. 223-1B). If the C7 plumb line is anterior to the posterior superior corner of the S1 vertebral body, the sagittal balance measure is reflected as a positive value, and if posterior, it is reflected as a negative value. Radiographic assessment of suspected spinal deformity should include both PA and lateral views because kyphotic deformities, such as those associated with neuromuscular disorders, may also be accompanied by a scoliotic deformity and primary scoliotic deformities may also include a degree of kyphotic deformity.
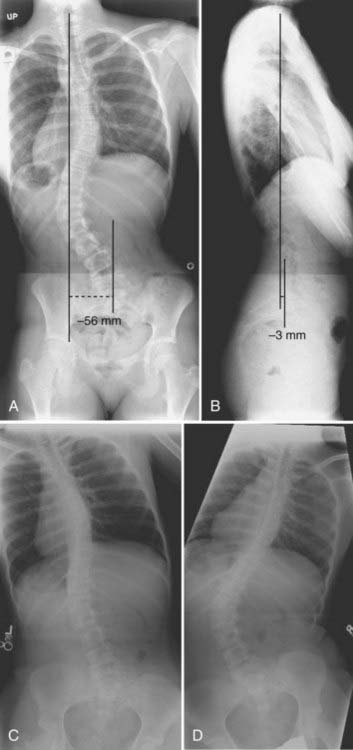
For patients with spinal deformity, radiographic imaging may also be beneficial in assessing the flexibility of deformities, which may prove useful for surgical planning. For example, the flexibility of scoliotic curves may be assessed with full-length PA supine radiographs in which the patient bends to the left side and to the right side (Fig. 223-1C and D). For patients who are not able to adequately cooperate with side-bending films, curve flexibility may be assessed with the patient placed over a bolster or with the use of traction. Similarly, the flexibility of kyphotic deformities may be assessed with a bolster placed under the apex of the kyphosis, and the flexibility of lordotic deformities may be assessed with the spine and pelvis placed in flexion.
Computed tomography (CT) can provide greater detail of bone anatomy and, with reformatted multiplanar images, can provide a three-dimensional view of complex deformities.3,4 Congenital deformities may have underlying anomalies, such as a hemivertebra or unsegmented bars, that may not be readily discernible on plain radiographs but can often be clearly defined with CT. The dimensions of the bony anatomy, such as pedicles and vertebral bodies, are also best assessed with CT, and such information may facilitate planning of surgical treatment, including selection and placement of implants.
Magnetic resonance imaging (MRI) is commonly used for the assessment of suspected pediatric spinal conditions. In the setting of spinal deformity, MRI can be used to evaluate for canal and foraminal stenosis, as well as for underlying abnormalities that may warrant treatment or affect surgical planning. For example, intraspinal deformities, such as tethered cord, syringomyelia, and tumors, have been reported in 15% to 38% of patients with congenital spinal deformity.5–10 Although MRI is often incorporated into the imaging evaluation of pediatric spinal deformity, certain findings should prompt special consideration for such evaluation. These findings include (1) pain that is severe; (2) neurological abnormalities, including motor weakness, muscle atrophy, and upper motoneuron signs; (3) early-onset scoliosis with a Cobb angle greater than 20 degrees; (4) atypical scoliosis curve patterns, such as left thoracic curves, sharp angular curves, congenital deformities, and curves greater than 70 degrees; (5) scoliosis curves with rapid progression (>1 degree per month); (6) neurofibromatosis patients to evaluate for an underlying neoplastic process; (7) deformity in the setting of myelomeningocele; and (8) absence of apical lordosis in patients with idiopathic scoliosis.1,11
Progression of deformity in the pediatric spine is typically related to the degree of skeletal maturity, with greater remaining growth potential corresponding to a greater risk for progression of deformity. Thus, assessment of skeletal maturity can provide prognostic information. Several methods for this assessment have been reported, including the Risser stage, closure of the triradiate cartilage, and hand films.1,12–15 The Risser stage reflects the degree of iliac ossification and is based on the proportion of the iliac crest that has undergone ossification. The Risser stage has been used historically to estimate skeletal maturity and remaining growth potential, with stages 1 through 4 corresponding to sequential ossification of each quarter of the iliac crest from anterior to posterior.16 Once stage 4 is reached, spinal growth is generally considered to be complete. Closure of the triradiate cartilage of the pelvis has also been correlated with the completion of spinal growth. Alternatively, hand films can be obtained for assessment of skeletal maturity without the need to expose the pelvis to radiation, as required for both the Risser stage and assessment of the triradiate cartilage.1,14
The rib-vertebral angle difference (RVAD) of Mehta is another example of an imaging study that can affect decision making in pediatric spinal deformity. This measure is an important prognostic indicator for infantile scoliosis.17 The RVAD is the difference between the angles formed by a line along the rib head and a perpendicular to the base of the apical vertebra on the right and left sides of the spine. Spontaneous resolution of the scoliosis is expected in 85% to 90% of patients if the RVAD is less than 20 degrees, whereas an RVAD of greater than 20 degrees suggests a high likelihood of curve progression.17
Congenital Disorders
Because of the complexity of embryogenesis, a broad range of congenital spinal disorders can develop.18 Although many congenital spinal disorders may not be evident at birth, each is thought to result from errors that occur during embryogenesis.19 Congenital spinal anomalies most commonly occur as sporadic events and are relatively uncommon, with an incidence of approximately 1 per 1000 to 2000 individuals in the general population.20–22 However, not all congenital spinal disorders are sporadic. For example, spinal dysraphism occurs in approximately 0.1% to 0.2% of individuals in North America, but the incidence in subsequent offspring increases to 2.5%,23 thus suggesting environmental, genetic, epigenetic, or other factors.
Congenital spinal malformations are not infrequently accompanied by other congenital anomalies, with the most common organ systems affected being those developing at a similar phase of embryogenesis. The urologic system is the most common system affected, with a reported incidence of up to 25%.24 The cardiovascular system demonstrates anomalies, including ventricular septal defects, atrial septal defects, dextrocardia, and the tetralogy of Fallot, in up to 10% of patients. Basu and colleagues evaluated 126 consecutive patients with congenital spinal deformity for evidence of intraspinal anomalies, as well as for defects in other organ systems.5 More than a third (37%) of the patients were found to have intraspinal abnormalities, and more than half (55%) were found to have other organic defects, including cardiac defects in 26% and urogenital abnormalities in 21%.
Congenital Scoliosis
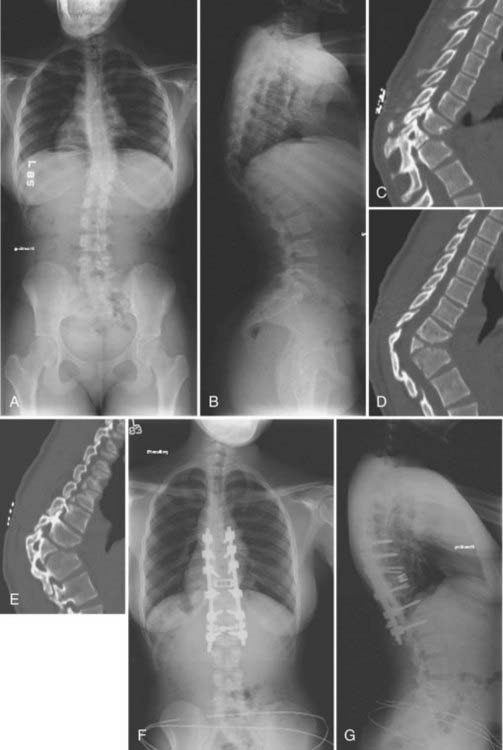
Scoliosis is an abnormal curvature of the spine in the coronal plane. Congenital scoliosis is distinguished by the presence of anomalous vertebrae at birth (Fig. 223-2). Although the vertebral abnormality is present at birth, typically no evidence of deformity is noted until the growth phases of childhood or adolescence. Relatively balanced spinal anomalies may even go undetected until adulthood or only be found incidentally. Infantile idiopathic scoliosis and juvenile idiopathic scoliosis are also manifested as scoliosis in childhood, but these types are distinguished from congenital scoliosis by their lack of vertebral anomalies.25

The clinical findings in patients with congenital scoliosis are highly varied and depend on the type and vertebral level of the spinal anomaly, the number of anomalies, and the degree to which the anomalies result in either cumulative global balance or imbalance. At the extremes, the anomalies can result in rapidly progressive scoliosis with significant morbidity in early childhood or can result in minimal or no deformity throughout life. Approximately a quarter of patients with congenital scoliosis can be expected to not progress, approximately half progress slowly, and the remaining quarter progress rapidly.18 With advancements in CT and MRI have come improvements in the ability to classify congenital scolioses, as well as improvements in the ability to optimize the planning and timing of therapeutic management.
Congenital abnormalities of the spine are classified according to the embryologic development of the spine, with categories including failure of formation, failure of segmentation, and mixed anomalies.1,26 Failure of formation ranges from mild wedging to complete absence of a vertebra. The most common cause of congenital scoliosis is a hemivertebra, which typically consists of a wedged vertebral body with a single pedicle and hemilamina. Segmentation failure results in unilateral or bilateral fusion of vertebrae.27,28 A unilateral unsegmented bar, which consists of a bony block that includes the disk space and facet joints, is the most common segmentation failure. Among the various complex combinations of vertebral anomalies that can coexist is an unsegmented bar with a contralateral hemivertebra, which can result in severe progressive scoliosis.29
An understanding of the natural history of congenital spinal anomalies is important to define the optimal treatment strategies. McMaster and Ohtsuka reported a series of 202 patients with congenital scoliosis and noted that 11% did not progress, 14% had limited progression, and 75% progressed significantly.25 The type of anomaly is an important factor with regard to progression. The most severe congenital scoliosis may result from a unilateral unsegmented bar with a contralateral hemivertebra at the same level. The significant potential for this combination of anomalies to produce deformity argues in favor of treating the patient immediately without allowing a period of observation.25,30 Patient age is also an important factor in determining the capacity for progression of deformity, with the greatest risk typically occurring during the preadolescent growth spurt. Children in whom the deformity develops in the first years of life often have considerable growth imbalance and are at high risk for significant deformity.
In children with severe or progressive congenital scoliosis, surgery is frequently the most effective treatment. Surgical options include hemivertebra excision, convex hemiepiphysiodesis, fusion in situ, spinal instrumentation, and thoracoplasty with a vertical expansion prosthetic titanium rib (VEPTR).18 Hemivertebra excision offers the ability to directly address the biomechanical decompensation and can provide immediate and often significant correction of the deformity.31–33 Convex hemiepiphysiodesis involves excision of the disk and fusion on the convex side of the curve and relies on the remaining growth potential on the side of the concavity.34 Although fusion in situ with casting or a brace has historically been popular, the use of posterior instrumented arthrodesis has become more popular in those requiring fusion. Patients with progressive curves and congenital rib fusions may benefit from thoracoplasty with a VEPTR.35,36 It is important to recognize the surgical morbidity that can accompany complex reconstructions for congenital scoliosis. Reames and coauthors reported a modern series of more than 2000 patients from the Scoliosis Research Society treated for congenital scoliosis; the morbidity rate was higher than 10% and mortality was 0.3%.37
Congenital Kyphosis
Congenital kyphosis is a deformity in the sagittal plane that results from vertebral anomalies, including failure of formation and segmentation (Fig. 223-3).1 Left untreated, congenital kyphosis often results in neurological deficits. Winter and colleagues reported a classification system for congenital kyphosis in which three types are distinguished: failure of formation of the vertebral body (type I), failure of segmentation of the vertebral body with a ventral unsegmented bar (type II), and mixed failure of formation and segmentation (type III).38 The most common form, type I, is also the most common type to result in severe deformity and neurological deficits, with the severity of deformity being related to the magnitude of the failure of formation. Type II produces less deformity and is considerably less likely to result in a neurological deficit. The severity of kyphosis produced with type II depends on the difference between ventral vertebral growth and growth of the dorsal structures. Type III is very rare and is thought to behave in a similar fashion as type I.
In general, nonoperative treatment is not recommended for congenital kyphosis because of the significant potential for the development of neurological deficits with progression. Generally, posterior fusion alone is adequate in patients who are younger than 5 years and have less than 55 degrees of kyphosis. Combined anterior and posterior procedures are often required in older patients and in those with greater than 55 degrees of kyphosis. Substantial risks for morbidity and mortality can be associated with surgical correction of congenital kyphosis. Kim and coauthors reported that complications are more likely to occur in the setting of kyphosis greater than 60 degrees and in patients in whom preoperative imaging demonstrates cord compression.39
Congenital Lordosis
Congenital lordosis results from dorsal defects in segmentation and is considerably rarer than either congenital scoliosis or congenital kyphosis.40 Congenital lordosis is often accompanied by a deformity in the coronal plane (lordoscoliosis) that results from a dorsolateral location of the unsegmented bar. The incidence of neurological deficits in patients with congenital lordosis is substantially lower than that in patients with congenital kyphosis. Instead, the most significant complications of congenital lordosis often relate to impairment of pulmonary function when the deformity occurs in the thoracic region.
Congenital Stenosis
Congenital spinal stenosis is considerably less common than the degenerative spinal stenosis that afflicts the adult population, although the congenital abnormality may remain essentially asymptomatic until adulthood. Congenital spinal stenosis is distinguished from developmental spinal stenosis by the latter usually occurring in conjunction with conditions such as achondroplasia, hypochondroplasia, diastrophic dwarfism, Morquio’s syndrome, and hereditary multiple exostoses.18 Verbiest has described three types of congenital spinal stenosis.41–43 The first type occurs together with a spinal dysraphism. The symptoms typically reflect a combination of the two conditions, and it is not uncommon for severe radicular symptoms and deficits to occur.
Verbiest’s second type of congenital spinal stenosis occurs as a result of failure of vertebral segmentation.41–43 A reduced midsagittal diameter of the vertebral canal frequently occurs in the area of the block vertebrae. The signs and symptoms are similar to those observed with idiopathic developmental spinal stenosis.
Verbiest’s third type of congenital stenosis results in an intermittent stenosis syndrome (d’Anquin’s syndrome).41–43 In this type, the spinous process of S1 is absent, and a central cleft exists in the S1 lamina. A hook-like process of L5 may protrude through this cleft when the patient assumes a standing posture and result in reduction of the midsagittal diameter of the sacral canal. Thus, the patient experiences radicular symptoms with standing and walking that are relieved with sitting.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


