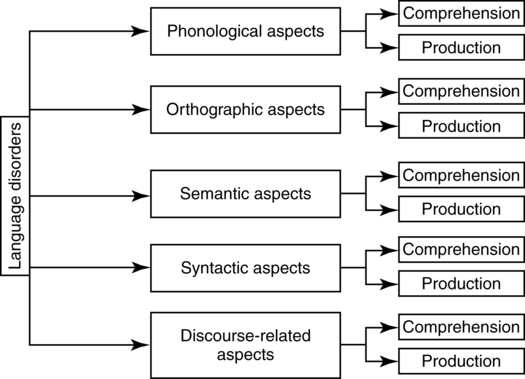
CHAPTER 14 Swathi Kiran and Chaleece Sandberg This chapter will first highlight the primary communication characteristics resulting from disturbances within the domain of language. Several sub-domains of language are elaborated, namely comprehension and production of phonological, orthographic, semantic, syntactic and discourse/pragmatic aspects of language (Figure 14-1). Next, general guidelines for assessment and some specific examples of currently used assessments will be discussed. Finally, an evidence-based review of the treatment literature for the last 10 years will be presented. From this review, effective treatment techniques for each type of impairment will be selected and described for use in clinical practice. The current chapter utilizes a theoretical framework presented by Ellis and Young (Ellis & Young, 1988) that is pertinent to comprehension and production of spoken and written words. Disorders specific to the semantic system will be discussed within interactive activation models (Dell, 1986) and syntactic disorders will be discussed within theoretical frameworks proposed by Garrett (1980) and Caplan (1992). Persons with impairment of the visual analysis system and visual input lexicon have difficulty decoding and recognizing written language, but may be able to correctly assign phonemes to orthography, using the grapheme-to-phoneme conversion route. This is considered to be a peripheral dyslexia called pure alexia or letter-by-letter reading. Other types of peripheral dyslexia include neglect dyslexia and attentional dyslexia, which result from cognitive impairments described in Chapter 8 of this book. Phonological dyslexia results from impairment of grapheme-to-phoneme conversion. These individuals are forced to rely on the whole-word semantic route and therefore read both regular and irregular real words with relatively high accuracy, but are unable to read nonwords and unfamiliar words. In contrast to phonological dyslexia, surface dyslexia results from impairment of the visual input lexicon and semantic system. These individuals exhibit impaired reading of irregular words, but preserved ability to read regular words and nonwords. Additionally, the person’s ability to retrieve the meaning of the word relies on his/her pronunciation such that stood may be read as stewed activating the meaning relating to food rather than the meaning related to position. Deep dyslexia is a manifestation of an impairment comprising both the semantic system and the grapheme-to-phoneme conversion mechanism. Persons with deep dyslexia produce semantic paraphasias and/or morphological errors; show effects of imageability, concreteness, and word class; and exhibit impairment reading nonwords, often substituting real words (e.g., bride for bripe). This section will describe aspects of deficits in language function that involve the semantic system and the processing of the meanings of words for comprehension and production. The semantic system receives input from several modalities: auditory verbal/nonverbal input, visual verbal/nonverbal input, tactile input, olfactory input, and gustatory input. These semantic representations appear to be organized within the semantic system hierarchically, but also in somewhat overlapping categories (Rogers & McClelland, 2003). Deficits in semantic processing, affecting either comprehension or production of language, can be modulated by psycholinguistic factors and semantic category factors. Psycholinguistic factors that affect linguistic performance include imageability, concreteness, familiarity, frequency, age of acquisition, and word class (Luzzatti, Raggi, Zonca, et al., 2002; Nickels & Howard, 1995). Semantic category factors include the category itself, animacy, and typicality (Kiran & Thompson, 2003a; Shelton & Caramazza, 1999). Based on the several studies that have examined semantic processing deficits in persons with aphasia, it is clear that a selective fractionation of the semantic system can occur resulting in specific loss of a semantic category, a certain hierarchical level of a category, the inputs and output modalities into the semantic system or in the automatic processes involved (read Shelton & Caramazza, 1999; Tyler & Moss, 2001). Access to the semantic system and activation within the semantic system can be explained via interactive activation models (Dell, 1986). Lexical access involves the following steps (Dell, 1986; Dell & O’Seaghdha, 1992; Dell, Schwartz, Martin, Saffran, & Gagnon, 1997). The semantic units receive external input (e.g., visual presentation of the picture cat). Activation spreads to all potential semantic nodes and down to the phonological units linked to those semantic nodes. The semantic and phonological units are connected bi-directionally, so semantic units receive input from activated phonological units. This positive feedback activates phonological neighbors of the target (e.g., mat, sat), semantic neighbors of the target (e.g., dog), and both semantically and phonologically related words (e.g., rat). The most highly activated word node is selected. A phonological frame is then activated, which represents the syllabic structure of the word, and is involved in the retrieval of phonemes. Interactive activation models are appealing because of their flexibility in explaining both comprehension and production impairments. Comprehension and/or production errors could result from incomplete/incorrect activation of semantic nodes, incomplete/incorrect activation of phonological nodes, or failures in the bi-directional links between the semantic and phonological nodes. Comprehension of sentences requires not only an understanding of the meanings of the words in the sentence, but also an understanding of how the relationships between words in a sentence influence the overall meaning of the message. While reading or listening to a sentence, the average reader/listener parses the sentence, assigning syntactic structure to its parts (e.g., noun, verb, etc.) and mapping thematic roles onto the syntactic structures (e.g., agent, theme, etc.). Generally, the comprehension of a sentence is affected by the type of verb (e.g., transitive, intransitive, dative) and the number of arguments (e.g., one place verb, two place verbs, three place verbs) (Shapiro, 1997). Further, sentences that require movement of a clause (e.g., It was the lady who the man kissed) are considered to be more difficult than canonical sentences (e.g., The man kissed the lady). Persons with agrammatism either cannot reliably use their syntactic parser or cannot reliably map thematic roles onto syntactic structures, or both (Caplan, Baker, & Dehaut, 1985; Schwartz, Linebarger, Saffran, & Pate, 1987). Often, these individuals rely on a heuristic route for sentence comprehension, using real world knowledge and canonical word order to extract meaning. Therefore, non-reversible sentences (e.g., The girl ate a cake) are easier to comprehend than reversible sentences (e.g., The girl pulled the boy) and canonical sentences (e.g., The boy kissed the girl) are easier to comprehend than noncanonical sentences (The boy was kissed by the girl). The production of a syntactically sound sentence as proposed by Garrett (1980) requires roughly six steps: (1) the formation of a message, (2) the assignment of thematic roles, (3) the selection of lexical items, (4) the assignment of syntactical and morphological items, (5) the selection of phonological forms, and (6) the planning of articulatory movements. Persons with agrammatism often omit function words and morphological endings during sentence production and may even have difficulty producing these forms during reading or repeating of single words. Persons with paragrammatism often make substitution errors with function words and morphological endings during sentence production. Further, paragrammatism may reflect a disturbance in the ability to monitor the speech planning process (Butterworth & Howard, 1987). The omission or substitution of function words and morphological endings suggests impairment of the assignment of syntactical and morphological items during sentence planning. Persons with agrammatism also exhibit reduced length and complexity in sentence production. Factors involved include reduced production of verbs, bias toward verbs that take fewer arguments (e.g., intransitive and transitive verbs, but rarely dative verbs), and reduced complexity of sentence structure (e.g., absence of embedded clauses) (Kim & Thompson, 2000; Thompson, Shapiro, Tait, Jacobs, & Schneider, 1996). Additionally, some agrammatic patients have difficulty generating logical relationships between lexical elements and may therefore produce sentences in which semantic aspects, such as animacy, influence word order rather than syntactic aspects, such as thematic roles (Saffran, Schwartz, & Marin, 1980). Recent studies have shown that patients typically classified as having Wernicke’s aphasia also show problems with assigning accurate syntactic information (Faroqi-Shah & Thompson, 2003), reaffirming the notion that classical aphasia syndromes do not always result in unique and nonoverlapping language characteristics. Discourse comprehension, or the ability to understand spoken or written text, requires a combination of language and cognitive skills for successful execution. In addition to the ability to understand the phonology, semantics, and syntax of the material, reasoning abilities such as drawing inferences and the ability to monitor information are needed to understand complex forms of discourse (Kamhi, 1997). In the process of reading or hearing a piece of discourse, the individual draws upon a range of skills including setting goals and expectations, problem solving, and shifting (van Dijk, 1987). An important aspect of conversational discourse is pragmatics. Conversation depends upon the ability for each conversational partner to understand the intended meaning of an utterance. This requires attention to the context in which the utterance is given, knowledge of each meaning that a word can have and assignment of the correct meaning to the correct context, and attention to visual (body language) and/or prosodic cues. The World Health Organization (WHO) International Classification of Functioning, Disability, and Health (ICF, http://www.who.int/classifications/icf/en/) is the international standard framework for describing health and disability. This classification system describes diseases/injuries using body function and structure, activity and participation, and environmental factors. Therefore, the main goals of assessment are to differentially diagnose the language disorder and to describe its relationship with body function and structure, how it will affect the patient’s activities and participation, and how environmental factors will affect recovery as well as activities of daily living. When choosing a test or battery of tests, it is good to begin with tests that give key information about all language modalities, such as the Western Aphasia Battery (WAB-R; Kertesz, 2006) or Boston Diagnostic Aphasia Examination (BDAE-3; Goodglass, Kaplan, & Barresi, 2000). The patient’s functional level can be determined with information from an initial patient or family interview or information from the referring specialist. When administering standardized tests, it is important to: (a) follow the test protocol, (b) administer all subtests, and (c) pace the testing according to the patient’s ability. Assessment of the integrity of the auditory phonological analysis system can be accomplished through the use of subtests such as those found in the Psycholinguistic Assessment of Language (PAL; Caplan & Bub, unpublished) and Psycholinguistic Assessment of Language Processing in Aphasia (PALPA; Kay, Lesser, & Coltheart, 1992). These tests utilize auditorily presented nonword minimal pairs and/or rhyming judgment to examine the patient’s ability to decode the word at the phoneme level. The use of nonwords ensures that the patient is not relying on the semantic system for decoding. Comparing performance on a nonword repetition task with performance on a real word repetition task can reveal problems with the link between the auditory analysis system and the phonological output buffer. A good test of the phonological input lexicon is an auditory lexical decision task compared to a visual lexical decision task. If the auditory lexical decision score is lower than the visual lexical decision score, but nonword repetition is intact, the deficit can be assumed to be at the level of the phonological input lexicon. Reading can be assessed with test batteries designed specifically for reading assessment, such as the Reading Comprehension Battery for Aphasia (RCBA-2; LaPointe & Horner, 1998) or the Gray Oral Reading Tests (although only standardized up to age 18) (GORT-4; Wiederholt & Bryant, 2001), or through subtests of other standardized measures, such as the PALPA. The goal of the reading assessment would be to identify the locus of the reading problem. Therefore, a compilation of tasks such as reading words that increase in letter length, reading regularly versus irregularly spelled words, reading pseudowords, and identifying pictures that match written words can help identify pure alexia, surface dyslexia, phonological dyslexia, and deep dyslexia. One way to determine the integrity of the semantic system without the confounding effects of deficits in reading, writing, auditory processing, or speech is through semantic judgment tasks. In these tasks, individuals are asked to judge the similarity of concepts represented by pictures. One such test is included in the Pyramids and Palm Trees Test (PAPT; Howard & Patterson, 1992). Poor performance suggests that the features of each concept that overlap are not available for analysis, indicating a disruption in the semantic system. Because anomia is a key feature of aphasia and language disorders in general, several tests are available to measure naming function. The Boston Naming Test (BNT; Goodglass, Kaplan, & Weintraub, 1983), the Test of Adolescent/Adult Word Finding (TAWF; German, 1990), and the Peabody Picture Vocabulary Test (PPVT-4; Dunn & Dunn, 2007)/Expressive Vocabulary Test (EVT-2; Williams, 2007) are a few of the tests specifically designed to measure naming. Many overall language batteries include subtests of naming objects, naming pictures, generating words in a category (e.g., animals, words that start with the letter _, etc.), and matching pictures to spoken or written words. It is important to include both spoken and written items to determine if the naming deficit is influenced by specific input or output modalities. Also, it is important to include animate and inanimate items, abstract and concrete items, items from different word classes, and items from several different semantic categories in order to determine whether or not the naming deficit is influenced by animacy, concreteness, imageability, word class, or semantic category. Other psycholinguistic factors to consider are word frequency, familiarity, and age of acquisition. Sentence comprehension can be measured through tests designed specifically for the purpose, such as the Auditory Comprehension Test for Sentences (Shewan, 1979), the Philadelphia Comprehension Battery (Saffran, Schwartz, Linebarger, et al., unpublished), and the Northwestern Sentence Comprehension Test (Thompson, unpublished-b). Subtests of the WAB, BDAE, PALPA, and PAL also measure sentence comprehension, as does the Revised Token Test (RTT; McNeil & Prescott, 1978). Sentence production can be measured through subtests of the PAL, or using subtests from the Northwestern Assessment of Verbs and Sentences (NAVS; Thompson, unpublished-a) that elicit specific sentence structures. In general, it is relatively easy for clinicians to obtain a narrative sample of a simple picture description task using pictures from the WAB, BDAE, or other material. Once the patient’s utterances are transcribed, the sentences/utterances can be subjected to a linguistic analysis of discourse (Saffran, Berndt, & Schwartz, 1989) in order to determine various aspects of syntactic structures. Conversational and monologic discourse can be assessed with nonstandardized techniques such as discourse analysis. In this technique, discourse is elicited through descriptive, narrative, procedural, or conversational tasks and analyzed using structured discourse analysis procedures. The Profile of Communicative Appropriateness (Penn, 1985) and Damico’s Clinical Discourse Analysis (1985) analyze pragmatic aspects of discourse, Quantitative Production Analysis (QPA, Saffran, et al., 1989) analyzes syntactic aspects of discourse, Correct Information Unit (CIU) analysis (Nicholas & Brookshire, 1993) measures the informativeness of discourse, and Type Token Ratio (TTR) is a measure of lexical diversity (see Malvern & Richards, 2002, for a discussion of D, which is a variant of TTR that can be used with large and varying sample sizes). Recently, Wright and colleagues (2008; 2005) developed an analysis of main events that measures a patient’s ability to provide the relationships and causation among elements in a story, above and beyond the informativeness and efficiency of the narrative. This analysis, in conjunction with a standard discourse analyses (e.g., TTR, CIU), shows promise as a sensitive tool for detecting treatment effects on narrative discourse in patients with aphasia. Comprehension of spoken and written discourse can be evaluated through the Discourse Comprehension Test (DCT; Brookshire & Nicholas, 1997). This test consists of spoken and written stories with corresponding questions that assess comprehension of directly stated and implied main ideas and details. Finally, functional communication can be assessed with formal measures, such as the Communication Activities of Daily Living test (CADL-2; Holland, Frattali, & Fromm, 1999) and Porch Index of Communicative Ability (PICA-R; Porch, 2001), or rating scales, such as the American Speech-Language-Hearing Association Functional Assessment of Communication Skills for Adults (ASHA FACS; Ferketic, Frattali, Holland, et al., 2003). Once a patient’s specific language impairments have been established, the overarching goal of treatment is to facilitate the general use of language for communication in order to increase the activities and participation of the patient. Treatment works toward reducing language impairment by increasing the efficacy of the residual language capacity and/or introduces compensatory strategies such as writing, drawing, or gesturing to aid the patient in conveying his/her message. Additionally, it may be helpful, especially for persons with progressive language disorders, to adapt the environment to facilitate better communication. For persons with non-progressive language disorders, the main goal of treatment should be to help him/her regain language function. Although compensatory strategies are important for the facilitation of communication, overreliance on them encourages learned nonuse of the impaired function (Taub et al., 1994). The patient’s physical and mental health status must be considered before beginning a therapy program. It is important to make sure that the patient is medically stable prior to beginning therapy in order to keep from doing harm to the patient by introducing too much stimulation (Holland & Fridriksson, 2001; Marshall, 1997). However, it is also important to take advantage of the spontaneous recovery that occurs within first few weeks after a brain injury to help maximize treatment effects (Hillis, 2005). In addition to considering aspects of the patient, aspects of the therapy programs that are available for use must also be considered. Do any of the available programs target your patient’s specific impairments? How effective is the therapy? Can it be modified to be more specific or more effective? Some programs will be perfect for your patient as is; others may need to be adapted for your patient’s specific needs or to increase the effectiveness of the chosen therapy program. Some programs are readily adaptable; others are not meant to be used in conjunction with other techniques. Two ways of adapting therapy for increased effectiveness are constraint-induced language therapy (CILT; alternatively referred to as CIAT (constraint-induced aphasia therapy) or intensive language-action therapy (Pulvermuller, Neininger, Elbert, et al., 2001) and the complexity account of treatment efficacy (CATE; Thompson, Shapiro, Kiran, & Sobecks, 2003). These techniques are discussed in detail in Box 14-1. In addition, the duration of treatment and frequency of treatment (number of sessions per week) need to be considered prior to beginning a therapy program. Generally, increasing the intensity of treatment (Bhogal, Teasell, & Speechley, 2003) and/or the complexity of the material being trained (Thompson, 2007) results in increased effectiveness of therapy. In the past 10 years, research of treatments for language disorders has flourished. Efficacy of existing treatments has been examined as well as exploratory research into new methodologies. This section will review the research literature from the past 10 years and suggest promising treatment methodologies. Treatment studies were retrieved from the Academy of Neurologic Communication Disorders and Sciences (ANCDS) Aphasia Treatment Website (www.aphasiatx.arizona.edu) as well as from the PubMed and PsychINFO databases. The studies reviewed below were evaluated by Beeson and colleagues based on guidelines described in their website (noted above). For a reader to judge the effectiveness of a treatment outcome in a research study, however, there are no clear metrics that are standardized across different studies. One approach is to evaluate the effect size of either the direct effect or the generalization effect. The direct effect is the effect on the actual trained material. This is similar to a final exam in most courses in which the material being tested is exactly the material that was covered in the course. The effect size is calculated by subtracting the average performance on the material before training from the average performance on the material after training and dividing by the standard deviation of the performance before training. The larger the effect size the more robust the treatment effect (for benchmarks specific to a treatment domain, see Beeson & Robey, 2008). The generalization effect is the effect that the training had on related, but untrained material. This is akin to taking the GRE (Graduate Record Examination) in which the material being tested is related to what you learned in your undergraduate coursework but may not be exactly the material that was covered in each of your courses. In patients with language disorders, generalization can be to standardized language tests or to a related, but different set of materials. The generalization effect size is calculated in the same manner as the direct effect size. It is helpful to keep this information in mind when reading treatment research articles. Treatments for pure word deafness and auditory phonological agnosia have not been well researched. Tessier and colleagues (2007) utilized an errorless learning paradigm to successfully train phoneme discrimination and recognition in a patient with word deafness. Stefanatos and colleagues (2005; 2008) recently proposed a temporal processing deficit in word deafness and suggested altering the rate of speech in treatment to facilitate the perceptual discrimination of speech. Phonological cueing hierarchies are a common method of training word retrieval and usually start with the first phoneme, then the first syllable, then repetition of the whole word, although they can be expanded to include nonword rhymes (Wambaugh, Linebaugh, Doyle, et al., 2001). This cueing technique for increasing word retrieval has been shown to be effective in isolation (Herbert, Best, Hickin, et al., 2001; Hickin, Best, Herbert, et al., 2002; Wambaugh, 2003; Wambaugh, Cameron, Kalinyak-Fliszar, et al., 2004; Wambaugh, Doyle, Martinez, & Kalinyak-Fliszar, 2002; Wambaugh et al., 2001) or when combined with orthographic, tactile, and/or semantic cueing hierarchies (Abel, Schultz, Radermacher, et al., 2005; Abel, Willmes, & Huber, 2007; Cameron, Wambaugh, Wright, & Nessler, 2006; Conroy, Sage, & Lambon Ralph, 2009; DeDe, Parris, & Waters, 2003; Fink, Brecher, Schwartz, & Robey, 2002). Another technique that can target phonological naming deficits is errorless learning (see Fillingham, Hodgson, Sage, & Ralph, 2003, for a review), which can simply be repetition of the target (Fillingham, Sage, & Lambon Ralph, 2005a, 2005b, 2006) or a reversed cueing hierarchy (Abel et al., 2005; Abel et al., 2007). Spaced retrieval is a form of errorless learning in which the repetition of a target is conducted over increasingly longer intervals and has recently been applied in patients with aphasia (Fridriksson, Holland, Beeson, & Morrow, 2005). Training specific phonological processes using tasks such as rhyming judgment, identifying the first/last phoneme, minimal pair discrimination, and segmenting/blending have also shown positive results for increasing naming (Corsten, Mende, Cholewa, & Huber, 2007; Franklin, Buerk, & Howard, 2002; Fridriksson et al., 2005; Kendall, Rosenbek, Heilman, et al., 2008; Laganaro, Pietro, & Schnider, 2003; Raymer & Ellsworth, 2002). Additionally, these types of treatments have been combined with gesture or semantic training (Rodriguez, Raymer, & Rothi, 2006; Rose, Douglas, & Matyas, 2002; Spencer et al., 2000). Phonological aspects of naming have also been trained through context, where pictures with phonologically similar names are presented simultaneously for confrontation naming (Fisher, Wilshire, & Ponsford, 2009). Similarly, contextual repetition priming is a treatment approach in which phonologically or semantically similar pictures are simultaneously and repeatedly presented for naming. Patients with phonological deficits generally appear to benefit more from this treatment than patients with semantic impairments (Martin, Fink, & Laine, 2004; Renvall, Laine, Laakso, & Martin, 2003). Some studies have shown better recovery of naming in persons with phonologically-based anomia after semantically focused training (Raymer, Kohen, & Saffell, 2006; Wambaugh et al., 2001). To summarize, when evaluating and developing treatment options for phonological impairments, it is advantageous to identify the locus of impairment prior to selecting a treatment strategy that is most applicable for the corresponding impairment (see Table 14-1 for examples of behavioral markers of phonological impairments and corresponding treatment strategies). Table 14-1 Behavioral Markers for Phonological Impairment and Corresponding Treatment Strategies
Treating communication problems in individuals with disordered language
Language disorders
Phonological aspects of language disorders
Comprehension
Orthographic aspects of language disorders
Comprehension
Semantic aspects of language disorders
Syntactic aspects of language disorders
Comprehension
Production
Discourse-related aspects of language disorders
Comprehension
Assessment
Overall goals of assessment
General guidelines of testing
Supplementary assessments: testing selective and specific language impairments
Phonological assessment
Comprehension
Orthographic assessment
Comprehension
Semantic assessment
Syntactic assessment
Comprehension
Production
Discourse assessment
Treatment
Overall goals of treatment
General considerations
Treatment research
Treatment for phonological impairments
Comprehension
Production
Behavioral Marker
Impaired phoneme discrimination
Pure word deafness—inability to identify spoken speech
Impaired segmenting/blending
Phonological paraphasias during naming, repeating, and reading
Impaired phonological processing abilities
Examples of Strategies for Use in Treatment of Phonological Impairments
Evidence
Rhyme judgment
Spencer et al. (2000), Franklin et al. (2002), Raymer et al. (2002), Doesborgh et al. (2004a)
Segmenting phonemes/syllables
Doesborgh et al. (2004a), Kendall et al. (2008)
Blending phonemes/syllables
Doesborgh et al. (2004a), Kendall et al. (2008)
Minimal pair discrimination
Corsten et al. (2007), Tessier et al. (2007)
Perceptual discrimination task
Stefanatos et al. (2005, 2008)
Monitor and correct phonetic speech errors
Franklin et al. (2002)
Phonological cueing hierarchy
Herbert et al. (2001), Wambaugh et al. (2001, 2003, 2004, 2007), Hickin et al. (2002), DeDe et al. (2003)
Phonological and orthographic cues
Fillingham et al. (2005a, 2005b, 2006)
Identify syllable structure/stress pattern
Rose et al. (2002)
Start with repetition and fade repetition cues (errorless learning and spaced retrieval)
Abel et al. (2005, 2007); Fridriksson (2005); Fillingham et al. (2005a, 2005b, 2006)
Phoneme identification
Franklin et al. (2002), Raymer et al. (2002), Corsten et al. (2007), Tessier et al. (2007), Kendall et al. (2008)
Provide pictures to name that are semantically or phonologically similar (contextual priming)
Martin et al. (2004); Renvall et al. (2003); Fisher et al. (2009) Related posts:
 The cognition of language and communication
The cognition of language and communication
 The effects of aging on language and communication
The effects of aging on language and communication
 The role of memory in language and communication
The role of memory in language and communication
 Management of acquired language disorders associated with attentional impairment
Management of acquired language disorders associated with attentional impairment
 Language and communication disorders associated with attentional deficits
Language and communication disorders associated with attentional deficits
 Attention: architecture and process
Attention: architecture and process
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree