Unilateral Cavernous Sinus Mass
Anne G. Osborn, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Pituitary Macroadenoma
Meningioma
Schwannoma
Metastases, Skull and Meningeal
Lymphoma, Metastatic, Intracranial
Nasopharyngeal Carcinoma
Less Common
Saccular Aneurysm
Carotid-Cavernous Fistula, Traumatic
Thrombosis, Cavernous Sinus
Dermoid Cyst
Epidermoid Cyst
Neurosarcoid
Pseudotumor, Intracranial
Hemangioma
Rare but Important
Plexiform Neurofibroma
Chordoma
Tuberculosis
Iatrogenic
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Lateral dural walls of cavernous sinuses (CSs) should be flat or concave on axial/coronal imaging
Convex outer margin indicates abnormality
Lateral dural wall thick, easy to see; medial = thin, difficult to delineate
CSs are septated (not single pool of venous blood)
CSs enhance strongly but contain normal filling “defects” (Meckel cave, cranial nerves, ICA)
If mass present, is it intrinsic or extrinsic to cavernous sinus?
Where does mass originate?
Sella: Pituitary macroadenoma
Sphenoid sinus/central skull base: Metastasis, nasopharyngeal carcinoma
Dura: Meningioma, hemangioma, pseudotumor
Does it contain “flow voids”?
Aneurysm
Dural AVF
Helpful Clues for Common Diagnoses
Pituitary Macroadenoma
Cavernous sinus invasion common with macroadenoma
Difficult to determine unless florid
Mass, gland indistinguishable (gland IS mass)
Meningioma
Diffusely infiltrates sinus, thickens dura
Lateral dural wall can sometimes be identified within thickened, intensely enhancing CS mass
Look for dural “tail” along clivus, tentorium
Look for other meningiomas (multiple meningioma syndrome)
Schwannoma
Most common = trigeminal, in Meckel cave
Typically well-marginated
Usually hyperintense on T2WI
Solitary > multiple (NF2)
Metastases, Skull and Meningeal
Three patterns
Hematogenous (direct or extension from skull base)
Perineural along cranial nerve (usually from nasopharyngeal or sinus tumor)
Direct geographic invasion (squamous cell, minor salivary gland tumors most common primaries)
Lymphoma, Metastatic, Intracranial
Primary CS rare; usually history of disease elsewhere
Nasopharyngeal Carcinoma
Two patterns
Direct cephalad extension into central skull base, CS
Perineural extension into cavernous sinus(es) along CNV2
Helpful Clues for Less Common Diagnoses
Saccular Aneurysm
Can be spontaneous, post-traumatic (pseudoaneurysm)
Can be patent or partially thrombosed
Prominent “flow void”, pulsation (phase) artifact
Carotid-Cavernous Fistula, Traumatic
Superior ophthalmic vein enlarged
± Basilar skull fracture
Usually at junction of vertical, horizontal ICA segments
Thrombosis, Cavernous Sinus
Nonenhancing thrombus, thickened enhancing dural walls
May be secondary to sinusitis (thrombophlebitis)
Superior ophthalmic vein(s) often enlarged
Proptosis common
Dermoid Cyst
Typically in Meckel cave, not CS proper
Fat density/signal intensity
Epidermoid Cyst
Typically in Meckel cave, not CS proper
CSF density/signal intensity
Usually occurs as extension from CPA lesion
Neurosarcoid
Can be uni- or bilateral
Look for thickened infundibular stalk, dural masses
Pseudotumor, Intracranial
Uni- > bilateral
Typically extends posteriorly from orbital apex into CS
Extensive dural enhancement along middle fossa can be present
Occasionally can be invasive, destructive; mimics neoplasm or aggressive infection
Hemangioma
True vasoformative neoplasm in CS, dura
May mimic meningioma
Helpful Clues for Rare Diagnoses
Plexiform Neurofibroma
Occurs only in NF1
Involves cutaneous, orbital branches of CN5
Infiltrative, unencapsulated mass
Look for
Scalp neurofibromas
Sphenoid wing dysplasia
Chordoma
Destructive mass, midline > lateral
Occasionally can originate in CS or extend asymmetrically from clivus into CS
Most are very hyperintense on T2WI
Tuberculosis
History of pulmonary TB
Dura-arachnoid thickening from basilar meningitis
Iatrogenic
Post-operative packing after trans-sphenoidal macroadenoma resection
Look for surgical defect in sellar floor
Caused by overpacking of defect
May appear very bizarre
Fat suppression sequence helpful
Image Gallery
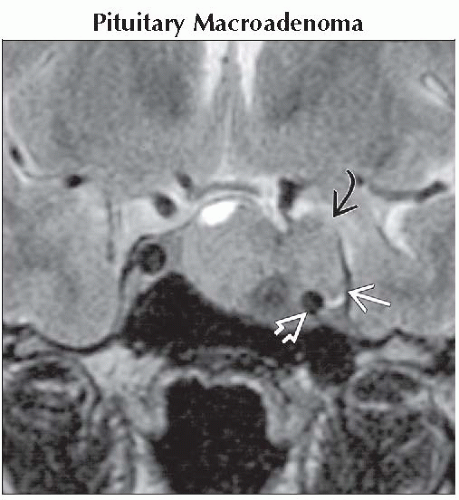 Coronal T2WI MR shows macroadenoma that extends into the left cavernous sinus
 , displacing and encasing the cavernous internal carotid artery , displacing and encasing the cavernous internal carotid artery  . The tumor lateral to the ICA . The tumor lateral to the ICA  confirms CS invasion. confirms CS invasion.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|