Chapter 51B Vascular Diseases of the Nervous System
Intracerebral Hemorrhage
Intracerebral hemorrhage (ICH) accounts for approximately 10% of strokes. Its clinical importance derives from its high frequency and 30-day mortality, which is close to 50%. There has been a general decline since the 1980s in the incidence of stroke, including ICH, as a result of improved detection and treatment of hypertension. However, ICH continues to be a major public health problem, especially in populations at high risk such as young and middle-aged blacks and Hispanics, in whom ICH occurs more frequently than in whites, and the medically indigent who lack hypertension treatment. A growing body of evidence suggests that genetic factors such as possessing the E2 and E4 alleles of the apolipoprotein E gene play an important role in the occurrence of certain forms of ICH such as lobar hemorrhages (O’Donnell et al., 2000). Novel potential genetic factors predisposing to ICH continue to be added by experimental and clinical studies (Gould et al., 2006). Finally, the management of ICH is controversial as the assessment of various interventions awaits the completion of prospective clinical trials.
Mechanisms of Intracerebral Hemorrhage
Hypertension
In one study of 188 patients with primary ICH (i.e., excluding patients with hemorrhage associated with ruptured arteriovenous malformations [AVMs], tumor, anticoagulant and thrombolytic therapy, and cocaine ingestion), it was determined that the cause was hypertension in 72% of patients. Further support for the importance of hypertension in the pathogenesis of ICH is the steady increase in ICH incidence with advancing age, which is also associated with an increase in the prevalence of hypertension. The role of hypertension as a cause of ICH is most relevant for the nonlobar locations, which may be due to hypertension in approximately 50% of cases (Woo et al., 2002). In both hypertensive and nonhypertensive patients, the circadian rhythm of ICH onset, with peaks at 8 am and 8 pm (Casetta et al., 2002), coincides with the physiological daily peaks of blood pressure, pointing to the importance of blood pressure rises in the pathogenesis of ICH.
The vascular lesion produced by chronic hypertension that leads to arterial rupture and ICH is probably lipohyalinosis of small intraparenchymal arteries. The role of microaneurysms of Charcot and Bouchard is uncertain, although their anatomical location at sites preferentially affected by ICH supports their causal importance. The nonhypertensive causes of ICH are listed in (Box 51B.1).
Box 51B.1 Nonhypertensive Causes of Intracerebral Hemorrhage
Vascular malformations (saccular or mycotic aneurysms, arteriovenous malformations, cavernous angiomas)
Bleeding disorders, anticoagulant and fibrinolytic treatment
Granulomatous angiitis of the central nervous system and other vasculitides, such as polyarteritis nodosa
Sympathomimetic agents (including amphetamine and cocaine)
Vascular Malformations
Because a detailed discussion of intracranial aneurysms and AVMs is provided elsewhere (see Chapter 51C), the analysis is limited here to the role of small vascular malformations in the pathogenesis of ICH. These lesions are often documented by magnetic resonance imaging (MRI), by pathological examination of specimens obtained at the time of surgical drainage of ICHs, or at autopsy. However, cerebral angiography also plays an important role in the diagnosis of these lesions. In a group of 38 young ICH patients (mean age 46 years) subjected to angiography, AVMs were documented in 23 patients and aneurysms in 9 (a total of 32 of 38, or 84%). The ICH in these 38 patients had computed tomography (CT) characteristics suggestive of an underlying structural lesion (associated subarachnoid or intraventricular bleeding, calcification, prominent vascular structures, atypical ICH location). However, in a group of 42 patients lacking these CT features, angiography still documented vascular abnormalities in 10 (AVMs in 8, aneurysm in 2) (Halpin et al., 1994).
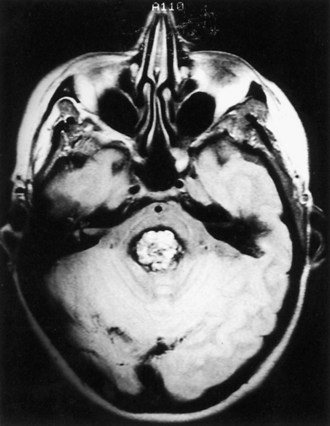
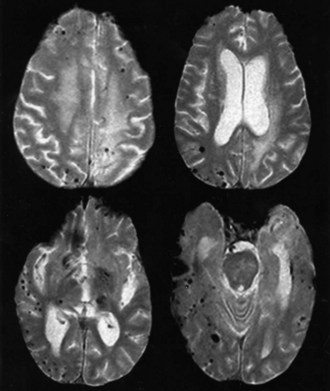
Cavernous angiomas are often recognized by MRI as a cause of ICH in the subcortical portions of the cerebral hemispheres and in the pons. This technique demonstrates a characteristic pattern on T2-weighted images, with a central nidus of irregular bright signal intensity mixed with mottled hypointensity (the “popcorn” pattern), surrounded by a peripheral hypointense ring corresponding to hemosiderin deposits (Fig. 51B.1), reflecting previous episodes of blood leakage at the edges of the malformation. These lesions are predominantly supratentorial, favoring the temporal, frontal, and parietal lobes, whereas the less frequent infratentorial locations favor the pons. They are generally single lesions, but multiplicity is not rare, especially in patients with familial cavernous angiomas. Familial clustering is common among individuals of Mexican descent, in whom cavernous angiomas are inherited in an autosomal dominant pattern linked to a mutation in chromosome 7q. Cavernous angiomas manifest with either seizures (27%-70%), ICH (10%-30%) or progressive neurological deficits (35%). ICH occurs in both the supratentorial and infratentorial varieties. A progressive course due to recurrent small hemorrhages within and around the malformation is occasionally seen in posterior fossa (especially pontine) lesions, and the deficits can evolve over protracted periods, at times suggesting a diagnosis of multiple sclerosis or a slowly growing brainstem tumor.
Intracranial Tumors
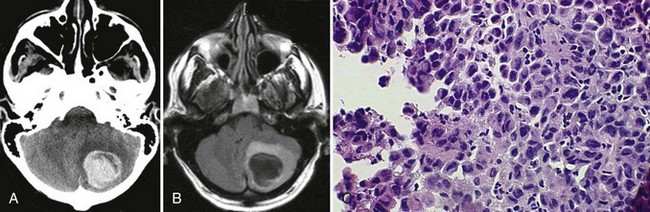
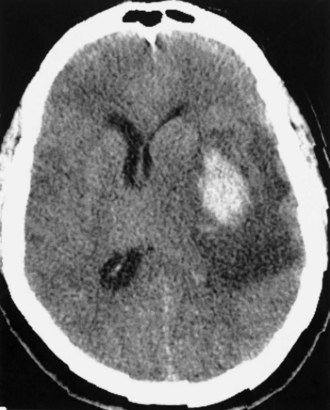
Bleeding into an underlying brain tumor is relatively rare in series of patients presenting with ICH, accounting for less than 10% of the cases. The tumor types most likely to lead to this rare complication are glioblastoma multiforme or metastases from melanoma, bronchogenic carcinoma, choriocarcinoma, or renal cell carcinoma (Fig. 51B.2). The ICHs produced in this setting may have clinical and imaging characteristics that should suggest an underlying brain tumor, including: (1) the presence of papilledema on presentation, (2) the location of ICH in sites that are rarely affected in hypertensive ICH, such as the corpus callosum, which in turn is commonly involved in malignant gliomas, (3) the presence of ICH in multiple sites simultaneously, (4) a CT scan characterized by a ring of high-density hemorrhage surrounding a low-density center in a noncontrast study, (5) enhancing nodules adjacent to the hemorrhage on contrast CT or MRI, and (6) a disproportionate amount of surrounding edema and mass effect associated with the acute hematoma (Fig. 51B.3). In these circumstances, a search for a primary or metastatic brain tumor should follow and include evaluation for systemic malignancy; if there is none, cerebral angiography and eventually craniotomy for biopsy of the wall of the hematoma cavity should be considered. Confirmation of the diagnosis of ICH secondary to malignant brain tumor carries a dismal prognosis, with a 30-day mortality rate in the 90% range.
Bleeding Disorders, Anticoagulants, and Fibrinolytic Treatment
Treatment with oral anticoagulants increases the risk of ICH by 8- to 11-fold compared with individuals with otherwise similar risk factors for ICH who are not receiving anticoagulants. Anticoagulant-related cases account for 9% to 11% of ICH. Potential risk factors for intracranial bleeding in patients receiving anticoagulants include advanced age, hypertension, preceding cerebral infarction, head trauma, and excessive prolongation of the International Normalized Ratio (INR). The last factor plays a major role in the pathogenesis of ICH in patients receiving oral anticoagulants. In the secondary stroke prevention trial, SPIRIT (Stroke Prevention in Reversible Ischemia Trial), 651 patients assigned to warfarin treatment were maintained at an INR of 3.0 to 4.5, resulting in 24 instances of ICH (14 fatal), in comparison with 3 ICHs (1 fatal) in the group of 665 patients treated daily with 30 mg of aspirin (The Stroke Prevention in Reversible Ischemia Trial Study Group, 1997). These data further support the recommendation that oral anticoagulation in patients with cerebrovascular disease should aim at an INR of 2 to 3 to reduce the frequency of this complication. The presence of severe leukoaraiosis on CT is an additional factor that independently increases the risk of ICH in patients on oral anticoagulants (Smith et al., 2002).
These hemorrhages have certain distinctive clinical characteristics: they tend to present with a slowly progressive course, at times over periods as long as 48 to 72 hours, in contrast with the usually more rapidly evolving presentation of hypertensive ICH; hematomas in patients receiving anticoagulants reach volumes that are, on average, larger than those occurring in hypertensive ICH, in turn resulting in the higher mortality rate of approximately 65%; signs of systemic bleeding rarely accompany ICH in this setting. Anticoagulant-related ICH may represent bleeding from vessels different from those involved in ICH of hypertensive origin (Hart et al., 1995). Certain angiopathies with bleeding potential, such as cerebral amyloid angiopathy (CAA), may play a causal role in the ICHs that occur in patients treated with anticoagulants (Rosand et al., 2000).
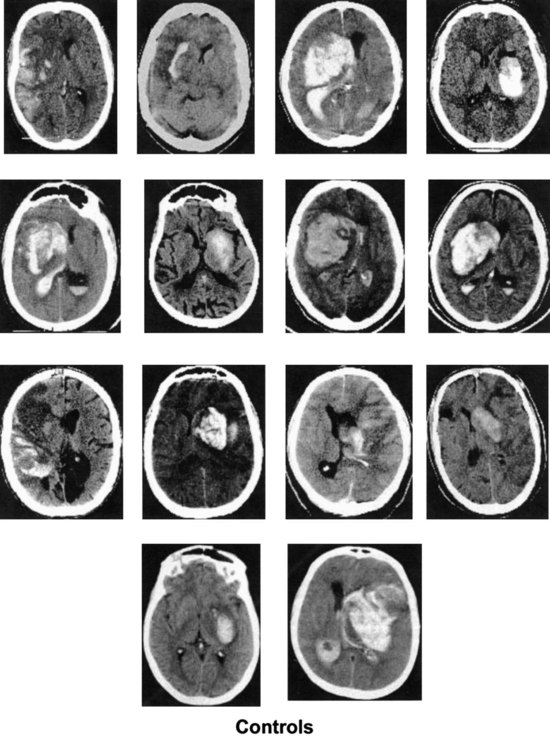
In addition to the anticoagulants, other substances with the potential for altering clot formation mechanisms are occasionally associated with ICH. These include drugs with fibrinolytic properties, such as streptokinase and tissue plasminogen activator (tPA). There is evidence to suggest that this complication of thrombolytic therapy may be favored by preexisting vasculopathies with bleeding potential such as CAA. Recombinant tPA for the treatment of acute ischemic stroke was complicated by ICH in 6.4% of cases (The National Institute of Neurological Diseases and Stroke [NINDS] rtPA Stroke Study Group, 1995), which is 10 times the rate found in the placebo group. Risk factors for ICH in this setting include a severe neurological deficit at presentation and documentation of hypodensity or mass effect on CT before treatment (The NINDS tPA Stroke Study Group, 1997). Intraarterial thrombolysis with prourokinase for middle cerebral artery occlusion leads to improved clinical outcomes but is associated with an 11% rate of early symptomatic ICH (Furlan et al., 1999). These hemorrhages occur at the site of the preceding cerebral infarct, are generally large (Fig. 51B.4), and carry a dismal prognosis (Kase et al., 2001). Hyperglycemia at pretreatment baseline has been identified as a potential risk factor for ICH in patients treated with either intraarterial prourokinase (Kase et al., 2001) or intravenous (IV) tPA (Bruno et al., 2002) for acute ischemic stroke. Another potential risk factor for ICH after intraarterial thrombolysis is the presence of incidental “microhemorrhages” (Fig. 51B.5), which can be easily detected with gradient echo (or “susceptibility-weighted”) MRI sequences (Kidwell et al., 2002). However, it is not yet clear whether these lesions are risk factors for postthrombolysis ICH; a large observational study failed to document such a relationship (Kakuda et al., 2005). Microhemorrhages are correlated with advancing age, ischemic stroke and ICH, as well as other manifestations of microangiopathy such as lacunar infarcts, leukoaraiosis, CAA, and the genetic disorder, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) (Viswanathan and Chabriat, 2006). The role of microhemorrhages in causing ICH after use of anticoagulants, antiplatelet agents, and thrombolytics has not been clearly defined by prospectively collected data. As a result, no recommendations can be given at present for using or withholding these treatment options based solely on the presence of these often incidentally detected lesions (Koennecke, 2006).
Granulomatous Angiitis of the Central Nervous System and Other Vasculitides
Granulomatous angiitis of the CNS, also referred to as isolated angiitis of the CNS, is characterized by mononuclear inflammation with giant cell formation in the media and adventitia of small and medium-sized intracranial arteries and veins (see Chapter 51E). An associated element of intimal hyperplasia leads frequently to cerebral infarcts and occasionally to ICH.
Among the vasculitides, the other variety that is known to present with ICH is polyarteritis nodosa. As opposed to granulomatous angiitis of the CNS, this form of necrotizing vasculitis depicts prominent signs of systemic involvement including fever, malaise, weight loss, anemia, elevated erythrocyte sedimentation rate, and renal impairment with hypertension (see Chapter 49A).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


