CHAPTER 208 Vein of Galen Aneurysmal Malformation
Vein of Galen aneurysmal malformations (VGAMs) are arteriovenous (AV) fistulas in the choroid fissure supplied by the choroidal arteries and draining to the dilated median vein of the prosencephalon, which is the precursor of the vein of Galen and the embryonic drainage of the choroid plexus. “VGAMs” were reported to represent less than l% of all arteriovenous malformations (AVMs) in the cooperative study of subarachnoid hemorrhage.1–3 However, its true incidence is difficult to determine because significant diagnostic confusion exists among the various malformations that cause dilation of the vein of Galen or its embryonic precursor. The embryonic nature of the draining veins of VGAMs was first described by Raybaud and colleagues in 1989.4 The concept of this disease was further refined by Lasjaunias and associates, who subclassified VGAMs into choroidal and mural types.5,6 Other vascular lesions that cause dilation of the true vein of Galen are designated as vein of Galen aneurysmal dilation (VGAD) or vein of Galen varix (VGV). VGAD is a group of malformations associated with dilation of the vein of Galen secondary to pial or dural AV shunts draining into the true vein of Galen or its tributary. VGV is a dilated vein of Galen without AV shunts.
Classification
Choroidal Vein of Galen Aneurysmal Malformations
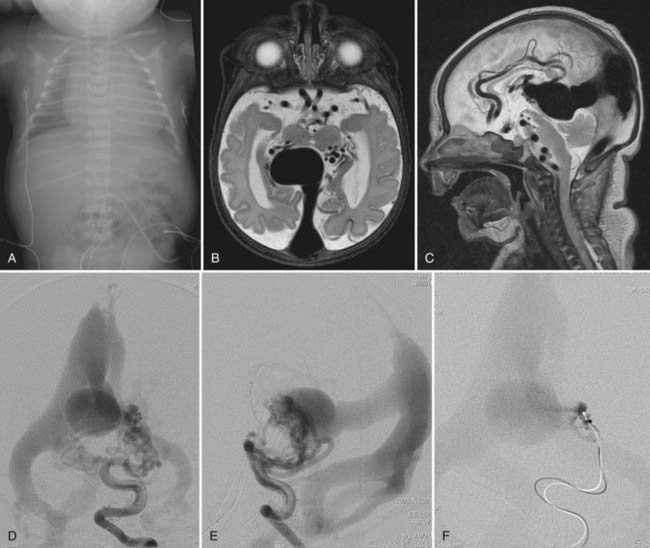
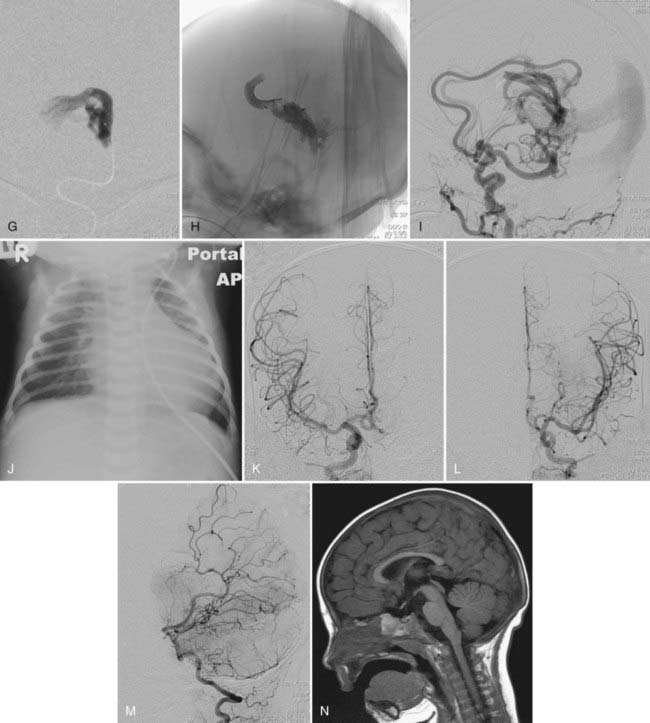
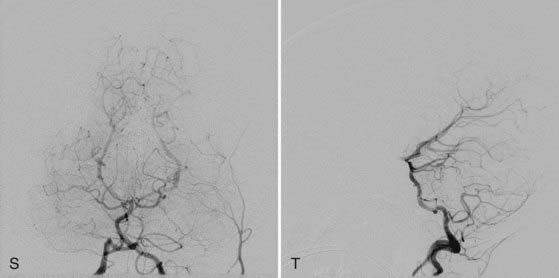
This more primitive type of VGAM consists of multiple fistulas located in the choroid fissure (Figs. 208-1 and 208-2). These multiple fistulas communicate with the anterior aspect of the median vein of the prosencephalon via an arterial network. The arterial feeders are all the choroidal arteries, including the bilateral anterior and posterior choroidal arteries, and the anterior cerebral arteries. There is often additional supply from the quadrigeminal and thalamoperforating arteries.4,7 The choroidal type of VGAM is the most severe expression of the disease and usually causes high-output cardiac failure in the newborn period because of multiple high-flow fistulas with less restriction of outflow than seen with the other type of VGAM. Choroidal VGAM is more challenging to treat because of comorbid conditions such as severe cardiopulmonary failure and the small size of the patient.
Mural Vein of Galen Aneurysmal Malformations
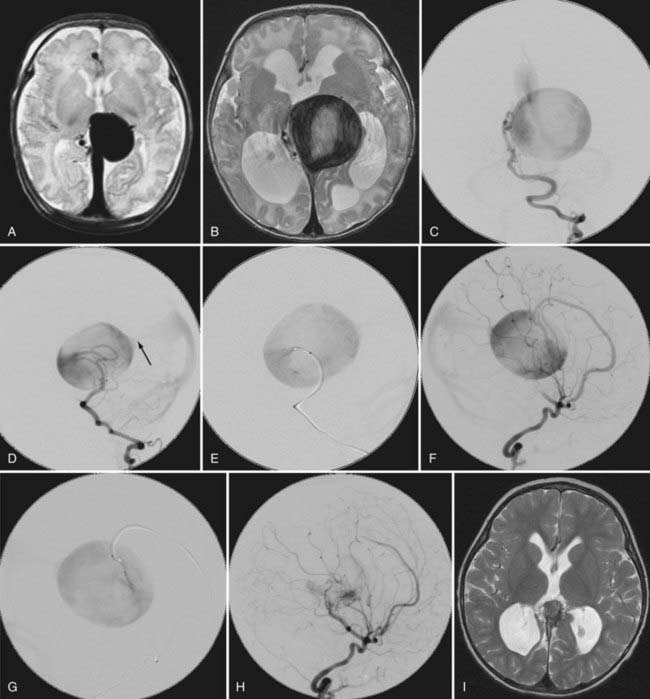
In mural VGAM, the fistulas are single or multiple and located at the wall of the dilated median vein of the prosencephalon, usually at its inferolateral margin (Fig. 208-3). The vessels supplying the shunt are usually the quadrigeminal or the posterior choroidal arteries (or both) and may be unilateral or bilateral. In contrast to choroidal-type VGAM, they have fewer fistulas and typically have more restriction of outflow, which causes more dilation of the median vein of the prosencephalon but protects the heart from high-output failure. The mural type of VGAM is therefore initially manifested later in infancy as macrocephaly, hydrocephalus, or failure to thrive, although it may be associated with mild cardiac failure or asymptomatic cardiomegaly.
Vein of Galen Aneurysmal Dilation
Pial Arteriovenous Malformation with Vein of Galen Aneurysmal Dilation
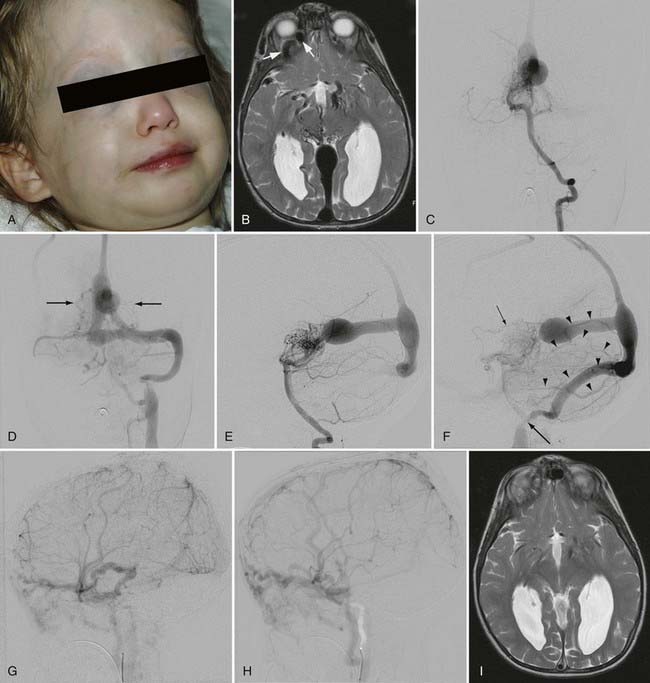
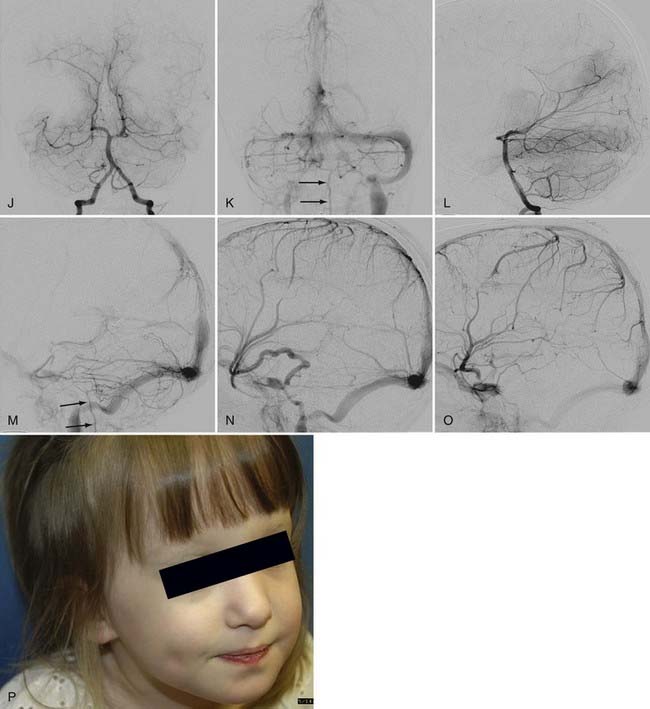
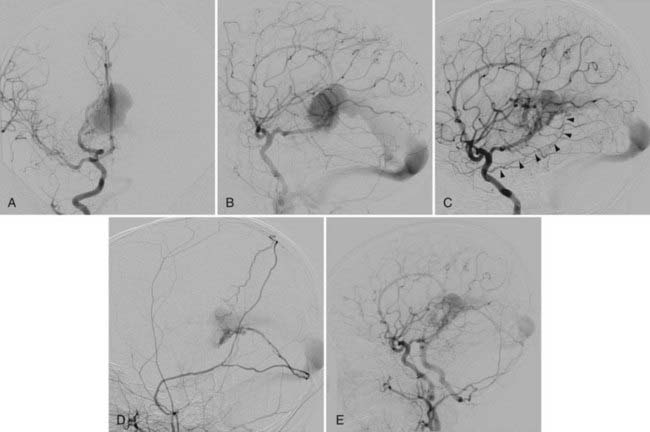
This type of VGAD is a pial or parenchymal AVM that drains into the dilated vein of Galen or its tributary (Figs. 208-4 and 208-5). Dilation of the vein of Galen is secondary to obstruction of outflow. The outflow obstruction can be relative and due to high-flow fistulas or absolute and due to progressive occlusion of the jugular bulb and the sigmoid sinus. Progressive occlusion of the dural sinus is frequently observed with pediatric fistulous malformations of the brain, including VGAM. The etiology of this outflow obstruction is unknown but may be related to underdevelopment of the jugular bulb, abnormal skull base maturation, and high-flow angiopathy of the venous system causing kinking or thrombosis at the tentorial or dural edge of the skull base. Because of this outflow restriction, the vein of Galen dilates and blood flow refluxes into other normal cerebral veins (the internal cerebral, vermian, hippocampal, basal, medial ventricular, parietal, and occipital veins or other normal tributaries of the vein of Galen). Patent embryonic sinuses such as the falcine sinus and the occipital sinus are often seen in both this type of VGAD and VGAM.
This type of VGAD is usually initially manifested in childhood or young adulthood as intracerebral hemorrhage, focal neurological deficit, or seizures. High-output cardiac failure can also occur in young children. Angiographic differentiation between VGAM and VGAD, especially a tectal AVM, can sometimes be difficult. Demonstration of transmesencephalic feeders by magnetic resonance imaging (MRI) or angiography confirms the pial nature of the lesion.8 Transmesencephalic feeders are projected below the P2 segment of the posterior cerebral artery on the lateral view of the vertebral artery angiogram.8 For treatment, transvenous occlusion of the venous dilation in the VGAD is contraindicated because it may produce hemorrhage or venous infarction of the deep cerebral structures as a result of occlusion of the outflow of these veins.
Dural Arteriovenous Malformation with Vein of Galen Aneurysmal Dilation
The dural AVM with VGAD is an acquired lesion in which AV shunts are located in the wall of the vein of Galen itself; it usually develops in the fourth or fifth decade of life. The vein of Galen dilation is due to stenosis or thrombosis of the straight sinus. Reflux is always noted into afferent cerebral veins from the vein of Galen. Typical clinical findings are headaches and progressive dementia secondary to cerebral venous hypertension. The arterial supply is derived predominantly from dural falcotentorial arteries from the internal and external carotid arteries and the vertebral artery, as well as the vasa vasorum to the wall of the vein of Galen from the pial arteries.9 Endovascular treatment of this type of dural AVM had been difficult because the transvenous approach is often not feasible and there are too many feeders from both the carotid and vertebral arteries for transarterial embolization. The recent introduction of Onyx (ev3, Irvine, CA) for embolization of dural AVMs has significantly improved the results of treatment of this type of dural AVM because a large volume of Onyx can be injected through one feeder to occlude an extensive dural vascular network supplied by multiple feeders and shunting to the dilated vein of Galen.
Vein of Galen Varix
VGV indicates dilation of the vein of Galen without the presence of an AV shunt. Two types have been encountered in children. One is transient asymptomatic dilation of the vein of Galen in neonates with cardiac failure from a cause other than VGAM. This dilation is usually noticed on an ultrasound study and disappears in several days after improvement of the cardiac condition. The second type of VGV occurs as an anatomic variation in which venous drainage of the brain converges toward the deep venous system. It is also asymptomatic, but this arrangement of venous drainage may predispose to future venous thrombosis and resultant ischemic symptoms because of the lack of compliance.7
In this chapter, we focus on the diagnosis and treatment of true VGAM.
Embryology
Expansion of the choroid plexus on the roof of the diencephalon induces the development of a midline dorsal vein draining the bilateral choroid plexuses. This vein is the first vein to drain an intracerebral structure and is designated the median vein of the prosencephalon. This vein remains functional during the second month and the first half of the third month of development. Progression of intracerebral vascularization and development of the basal ganglia result in formation of the paired internal cerebral veins, which then annex the venous drainage of the choroid plexus. This leads to regression of the median vein of the prosencephalon except for the most caudal portion, which joins with the internal cerebral veins to form the vein of Galen. Based on analysis of the vascular anatomy of VGAMs and vascular embryology, Raybaud and colleagues estimated that formation of the VGAM probably occurs between the embryonic stage of 21 to 23 mm (6 weeks) and 50 mm (11 weeks).4
Angioarchitecture of Vein of Galen Aneurysmal Malformations
VGAM, including the feeding arteries and the draining vein, exists in the subarachnoid space within the choroid fissure. The choroid fissure consists of the cistern of the velum interpositum and the quadrigeminal cistern. The arteries in the cistern of the velum interpositum are the choroidal arteries, including the anterior and posterior choroidal arteries, and the anterior cerebral arteries. The posterior choroidal arteries can have anastomoses among themselves without the existence of a VGAM. The anterior choroidal artery reaches the foramen of Monro along the choroid plexus. The anterior cerebral artery courses around the splenium of the corpus callosum anteriorly and supplies the choroid plexus at the foramen of Monro. The arteries in the quadrigeminal cistern are quadrigeminal (collicular) arteries coming off the posterior circle of Willis. They usually originate from the crural or ambient segment of the posterior cerebral artery, the superior cerebellar artery, and the medial posterior choroidal artery. They form a dense arterial network in the subarachnoid space above the quadrigeminal plate.4
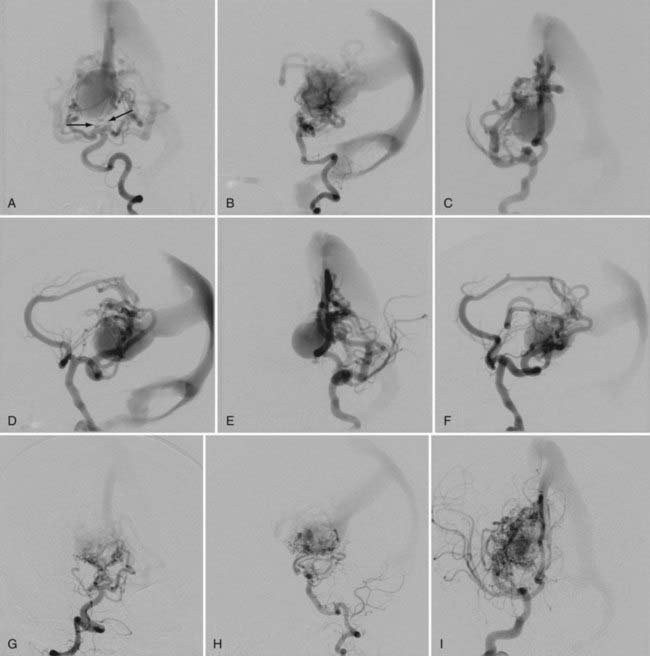
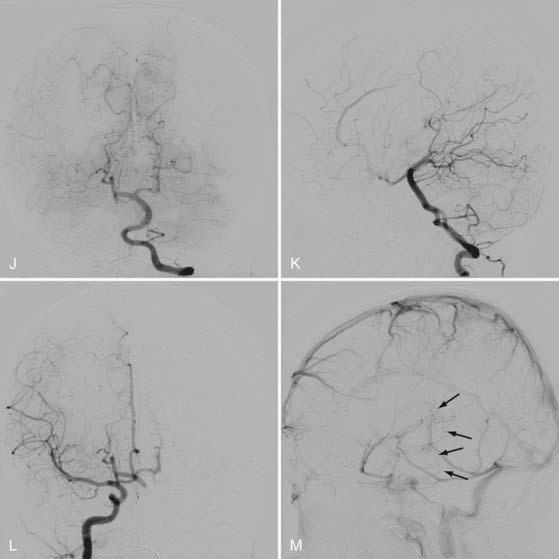
Other potential contributors to the VGAM include thalamoperforating and subependymal feeders from the posterior circle of Willis. They are secondary feeders because of the “sump” effect of the venous drainage and may regress after occlusion of the primary shunts (see Fig. 208-2). Dural feeders may exist or develop secondarily via the supply to the vasa vasorum at the venodural junction. The choroidal-type VGAM may form fistulas to the choroidal vein at the interventricular foramen and is supplied by perforators from the anterior cerebral artery or Heubner’s artery.7
The dilated draining vein of the VGAM is the embryonic median vein of the prosencephalon, as described in the embryology section. It is located in the midline and receives bilateral supply, although it may be shifted to one side, opposite the major fistula. A choroidal VGAM is more primitive and has multiple fistulas with an interposing arterial network between the feeders and the draining vein. The mural type has single or multiple fistulas on the wall of the dilated draining vein. Multiple feeders can converge into a common vascular channel opening into the dilated vein. A mixed malformation with features of both the choroidal and mural types may also occur.7
The median vein of the prosencephalon has no communication with the drainage system of the normal brain. The choroidal veins embryologically drain into the median vein of the prosencephalon and may remain connected to the median vein with or without the existence of fistulas to the choroidal vein itself. This connection is seen mostly with choroidal-type VGAMs and may mediate communication between the median vein of the prosencephalon and the striate vein, which may be a cause of hemorrhage or venous infarction after transvenous embolization of the VGAM. The straight sinus is absent with most VGAMs, and the dilated median vein of the prosencephalon usually drains to the embryonic falcine sinus, which connects to the posterior third of the superior sagittal sinus.10 Persistence of other embryologic sinuses, such as the occipital and marginal sinuses, is often observed in patients with VGAMs. Persisting arterial anomalies such as a limbic arterial ring involving the anterior and posterior choroidal arteries and pericallosal arteries are also frequently present.
Because of lack of connection to the median prosencephalic vein, the deep venous drainage of the brain takes an alternative pathway. The most commonly observed pattern of deep venous drainage is through the thalamic vein connecting to the lateral mesencephalic vein. This drainage system takes an epsilon shape and is seen to connect to the superior petrosal sinus on lateral angiographic views.10,11
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


