Chapter 5 Ventricular System and Cerebrospinal Fluid
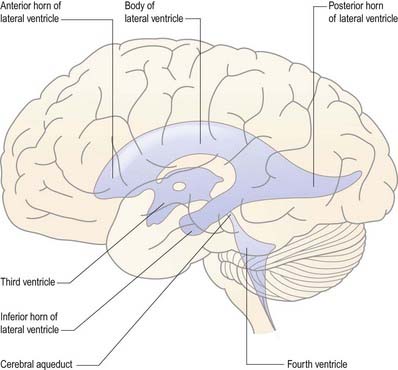
The cerebral ventricular system consists of a series of interconnecting spaces and channels within the brain that are derived from the central lumen of the embryonic neural tube and the cerebral vesicles to which it gives rise (Ch. 3). Within each cerebral hemisphere lies a large C-shaped lateral ventricle (Figs. 5.1, 5.2). Near its rostral end the lateral ventricle communicates through the interventricular foramen (foramen of Monro) with the third ventricle, which is a midline, slit-like cavity lying between the right and left halves of the thalamus and hypothalamus. Caudally, the third ventricle is continuous with the cerebral aqueduct, a narrow tube that passes the length of the midbrain; this, in turn, is continuous with the fourth ventricle, a wide, tent-shaped cavity lying between the brain stem and cerebellum. Caudally, the fourth ventricle is continuous with the vestigial central canal of the spinal cord.
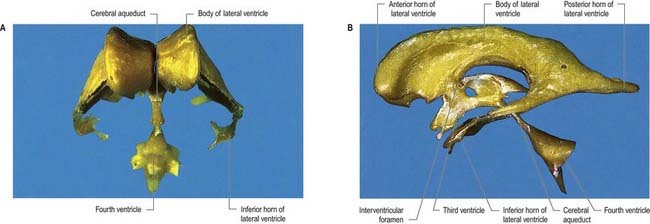
Fig. 5.1 Resin casts of the ventricular system of the human brain. A, Anterior view. B, Left lateral view.
(Prepared by D. H. Tompsett, Royal College of Surgeons of England.)
Topography and Relations of the Ventricular System
Lateral Ventricle
Viewed from its lateral aspect, the lateral ventricle has a roughly C-shaped profile, with an occipital tail (see Fig. 5.1). The shape is a consequence of the developmental expansion of the frontal, parietal and occipital regions of the hemisphere (Ch. 3), which displaces the temporal lobe inferiorly and anteriorly. Both the caudate nucleus and the fornix, which lie in the wall of the ventricle, have adopted a similar morphology, so the tail of the caudate nucleus encircles the thalamus in a C shape, and the fornix traces the outline of the ventricle forward to the interventricular foramen.
The lateral ventricle is customarily divided into a body and anterior, posterior and inferior horns (Figs. 5.1, 5.3). The anterior (frontal) horn lies within the frontal lobe. It is bounded anteriorly by the posterior aspect of the genu and rostrum of the corpus callosum, and its roof is formed by the anterior part of the body of the corpus callosum. The anterior horns of the two ventricles are separated by the septum pellucidum. The coronal profile of the anterior horn is roughly that of a flattened triangle in which the rounded head of the caudate nucleus forms the lateral wall and floor (Fig. 5.4). The anterior horn extends back as far as the interventricular foramen.
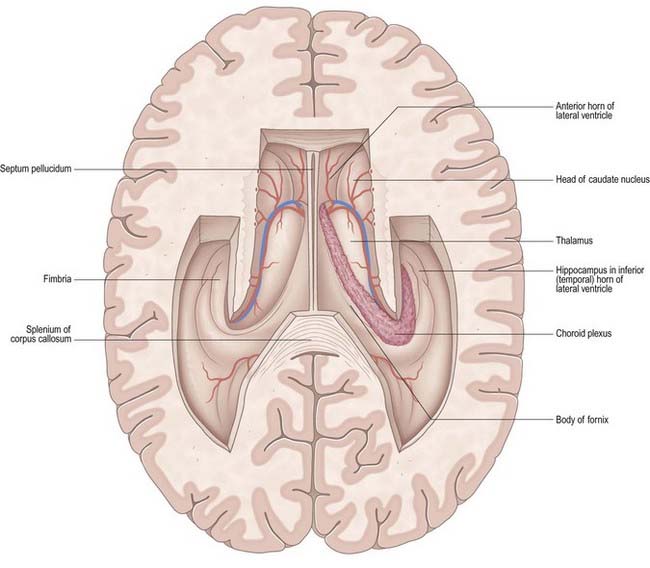
Fig. 5.3 Horizontal section of the cerebrum dissected to remove the roofs of the lateral ventricles.
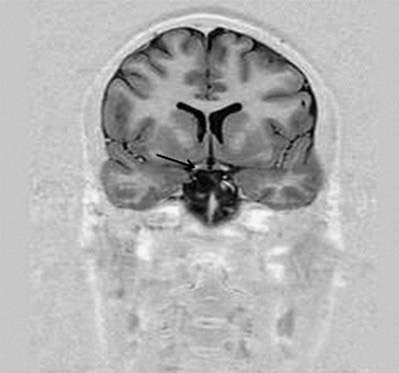
Fig. 5.4 Transverse MRI scan, at the level of the anterior horn of the lateral ventricle.
(Courtesy of Professor Alan Jackson, Department of Neuroradiology, University of Manchester, United Kingdom.)
The body lies within the frontal and parietal lobes and extends from the interventricular foramen to the splenium of the corpus callosum. The bodies of the lateral ventricles are separated by the septum pellucidum, which contains the columns of the fornices in its lower edge. The coronal profile of the body of the ventricle is a flattened triangle with an inward-bulging lateral wall, formed by the thalamus inferiorly and the tail of the caudate nucleus superiorly. The boundary between the thalamus and caudate nucleus is marked by a groove (see Fig. 5.3), which is occupied by a fascicle of nerve fibres, the stria terminalis, and the thalamostriate vein. The inferior limit of the body of the ventricle and its medial wall are formed by the body of the fornix. The fornix is separated from the thalamus by the choroid fissure. The choroid plexus occludes the choroid fissure and covers part of the thalamus and fornix. The body of the lateral ventricle widens posteriorly to become continuous with the posterior and inferior horns at the collateral trigone or atrium.
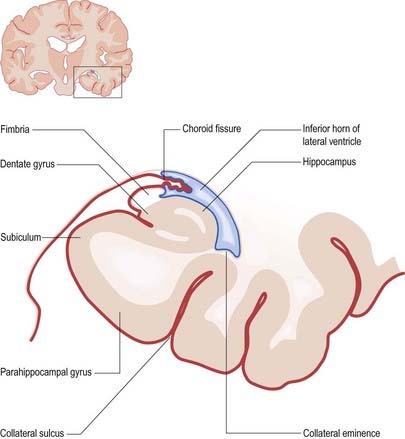
The floor of the ventricle consists of the hippocampus medially and the collateral eminence, formed by the infolding of the collateral sulcus, laterally. The inferior part of the choroid fissure lies between the fimbria (a distinct bundle of efferent fibres that leaves the hippocampus) and the stria terminalis in the roof of the temporal horn (Fig. 5.5). The temporal extension of the choroid plexus fills this fissure and covers the outer surface of the hippocampus.
Third Ventricle
The third ventricle is a midline, slit-like cavity derived from the primitive forebrain vesicle (Figs. 5.1, 5.2, 5.6–5.8). The upper part of the lateral wall of the ventricle is formed by the medial surface of the anterior two-thirds of the thalamus, and the lower part is formed by the hypothalamus anteriorly and the subthalamus posteriorly. An indistinct hypothalamic sulcus extends horizontally on the ventricular wall between the interventricular foramen and the cerebral aqueduct, marking the boundary between the thalamus and hypothalamus. Dorsally, the lateral wall is limited by a ridge covering the stria medullaris thalami. The lateral walls of the third ventricle are joined by an interthalamic adhesion, or massa intermedia, a band of grey matter that extends from one thalamus to the other.

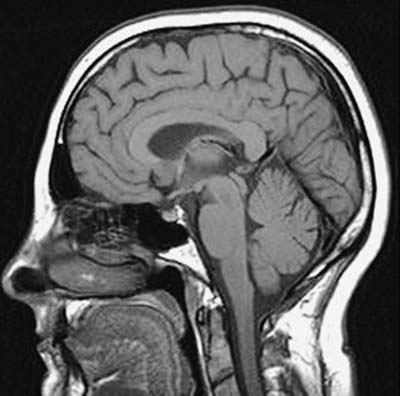
Fig. 5.7 MRI scan of the head in the sagittal plane.
(Courtesy of Professor Alan Jackson, Department of Neuroradiology, University of Manchester, United Kingdom.)
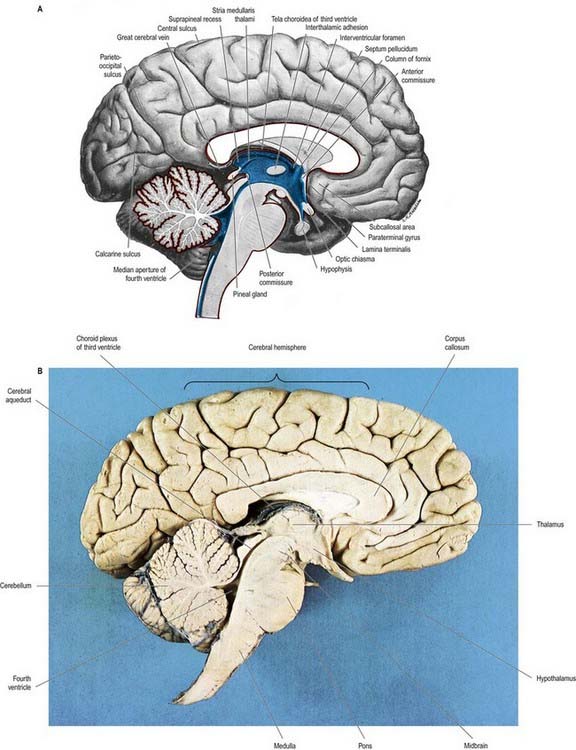
Fig. 5.8 A, Sagittal hemisection of the brain showing the third and fourth ventricles. Pia mater, red; ependyma, blue. B, Sagittal hemisection through the brain.
(Hemisection by E. L. Rees; photograph by Kevin Fitzpatrick on behalf of GKT School of Medicine, London.)
Anteriorly, the third ventricle extends to the lamina terminalis (see Fig. 5.8). This thin structure stretches from the optic chiasma to the rostrum of the corpus callosum and represents the rostral boundary of the embryonic neural tube. The lamina terminalis forms the roof of the small virtual cavity lying immediately below the ventricle, called the cistern of the lamina terminalis. This is important because it contains the anterior communicating artery, and aneurysm formation at this site may cause intraventricular haemorrhage through the thin membrane of the lamina terminalis. Above this, the anterior wall is formed by the diverging columns of the fornices and the transversely oriented anterior commissure, which crosses the midline. The anterior and posterior commissures are important neuroradiological landmarks. Before the introduction of modern imaging techniques, the anterior and posterior commissures could be identified by ventriculography. This led to their use as markers of the baseline for stereotactic surgical procedures. This convention is now universal, and the positions of the anterior and posterior commissures are the basic reference points for most surgical atlases of brain anatomy. The narrow interventricular foramen is located immediately posterior to the column of the fornix and separates the fornix from the anterior nucleus of the thalamus.
The roof of the third ventricle is a thin ependymal layer that extends from its lateral walls to the choroid plexus, which spans the choroid fissure (see Fig. 5.6). Above this is the body of the fornix. The posterior boundary of the ventricle is marked by a suprapineal recess above the pineal gland, by a pineal (epiphyseal) recess that extends into the pineal stalk and by the posterior commissure. Below the commissure, the ventricle is continuous with the cerebral aqueduct of the midbrain.
Cerebral Aqueduct
The cerebral aqueduct is a small tube, roughly circular in transverse section and approximately 2 mm in diameter. It extends throughout the dorsal quarter of the midbrain in the midline and is surrounded by the central, periaqueductal grey matter (see Fig. 5.8). Rostrally, it commences immediately behind and below the posterior commissure, where it is continuous with the caudal aspect of the third ventricle. Caudally, it is continuous with the lumen of the fourth ventricle at the junction of the midbrain and pons. The superior and inferior colliculi are dorsal to the aqueduct, and the midbrain tegmentum is ventral.
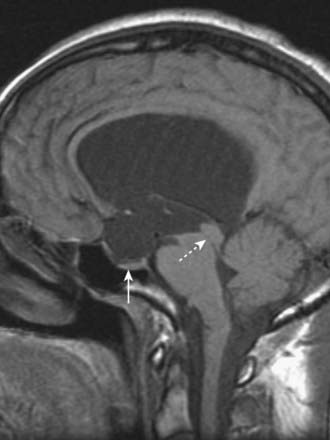
CASE 1 AQUEDUCTAL STENOSIS
Imaging demonstrates symmetric enlargement of the lateral and third ventricles (Fig. 5.9). The aqueduct is not visualized, and the fourth ventricle and cisterna magna are normal. A diagnosis of aqueductal stenosis is made, and ventricular shunting results in remarkable clinical improvement.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


