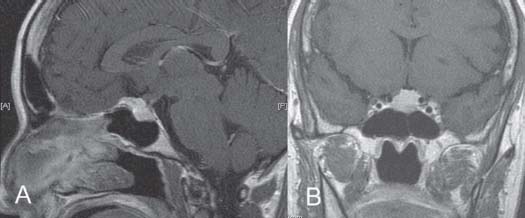
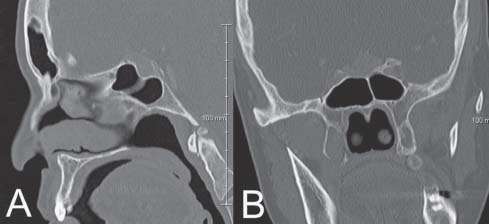
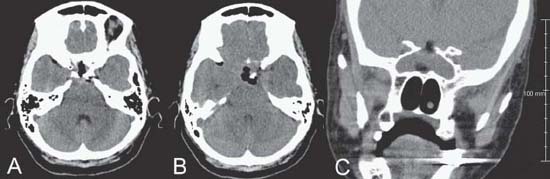
Case 12 Pituitary Adenoma Fig. 12.1 (A) Sagittal and (B) coronal T1-weighted magnetic resonance images with contrast demonstrating lesion at the level of the sella. Fig. 12.2 (A) A computed tomography scan of the head with sagittal and (B) coronal reconstructions demonstrating the same lesion in the sella and the sphenoid sinus anatomy at that level. Fig. 12.3 (A) A computed tomography scan of the head with axial images through the sella, (B) suprasellar, and (C) coronal reconstruction. Intrasellar and suprasellar air and fat graft are visualized. No intracranial hematoma or hydrocephalus is seen.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
12 Pituitary Adenoma
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


